
Neurotology — MCQs

On this page
All are true about Ramsay Hunt syndrome except?
What is the earliest ocular finding in acoustic neuroma?
What is the treatment of choice for acoustic neuroma?
Dehiscence of the anterior wall of the external auditory canal causes infection to the parotid gland. What is this condition known as?
A 70-year-old man presents with tinnitus. What is the most probable diagnosis?
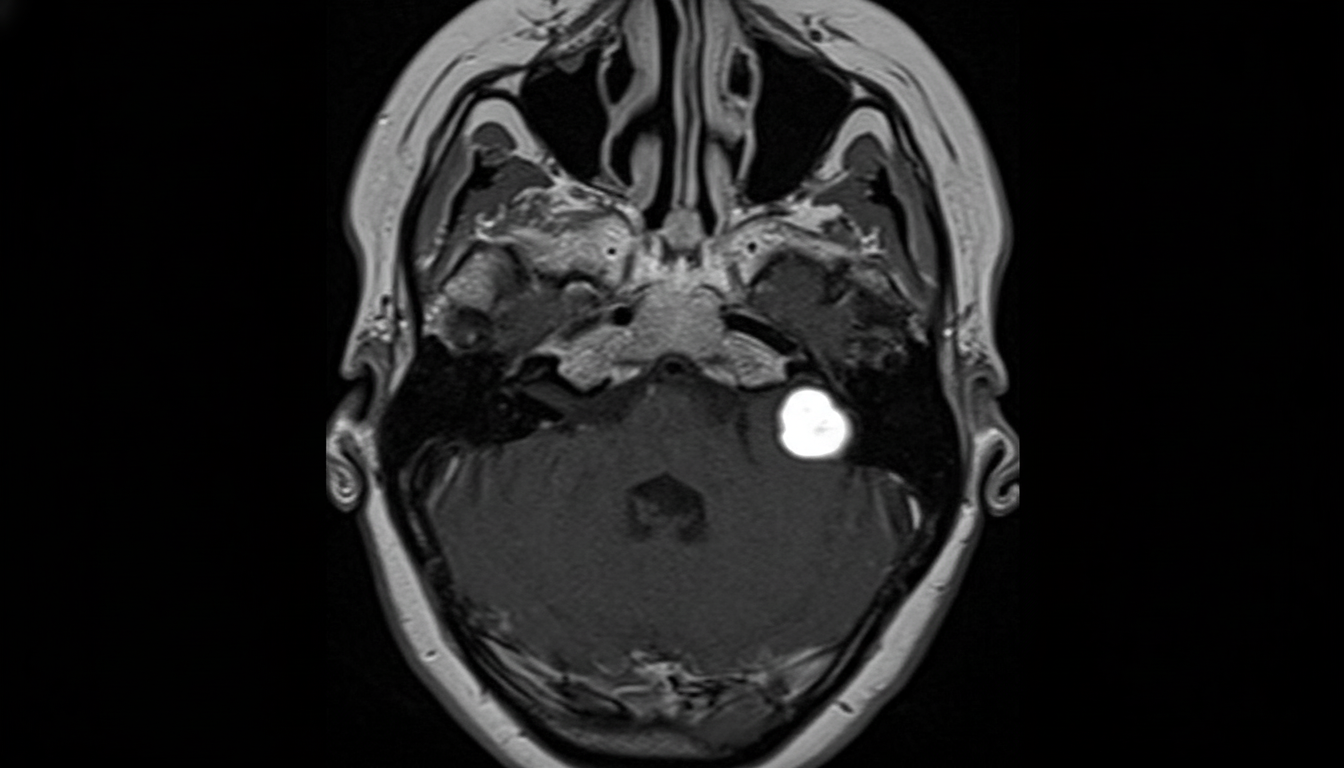
What is the investigation of choice for an acoustic neuroma of 1 cm diameter?
A patient presents with Bell's palsy. What is the initial treatment?
Pulsatile tinnitus in which condition is a common presentation?
Which of the following is NOT characteristic of Ramsay Hunt syndrome?
A triad of tinnitus, progressive deafness, vertigo, along with facial weakness is seen in which of the following conditions?
Practice by Chapter
Vestibular System Anatomy and Physiology
Practice Questions
Vestibular Testing
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Neuritis
Practice Questions
Labyrinthitis
Practice Questions
Acoustic Neuroma
Practice Questions
Other Cerebellopontine Angle Tumors
Practice Questions
Facial Nerve Disorders
Practice Questions
Skull Base Surgery
Practice Questions
Cochlear Implantation
Practice Questions
Vestibular Schwannoma Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app