
Neurotology — MCQs

On this page
What is the commonest cause of acute otitis media in children?
A child presents with ear infection with foul-smelling discharge. On further exploration, a small perforation is found in the pars flaccida of the tympanic membrane. What is the most appropriate next step in management?
The organ of Corti is situated in which of the following structures?
Which of the following is NOT caused by an acoustic neuroma?
What is the cause of myringosclerosis?
What is the average length of the adult external auditory canal?
What is the cause of unilateral secretory otitis media in an adult?
The Arnold nerve is a branch of which of the following nerves?
All of the following are of the size of an adult ear except?
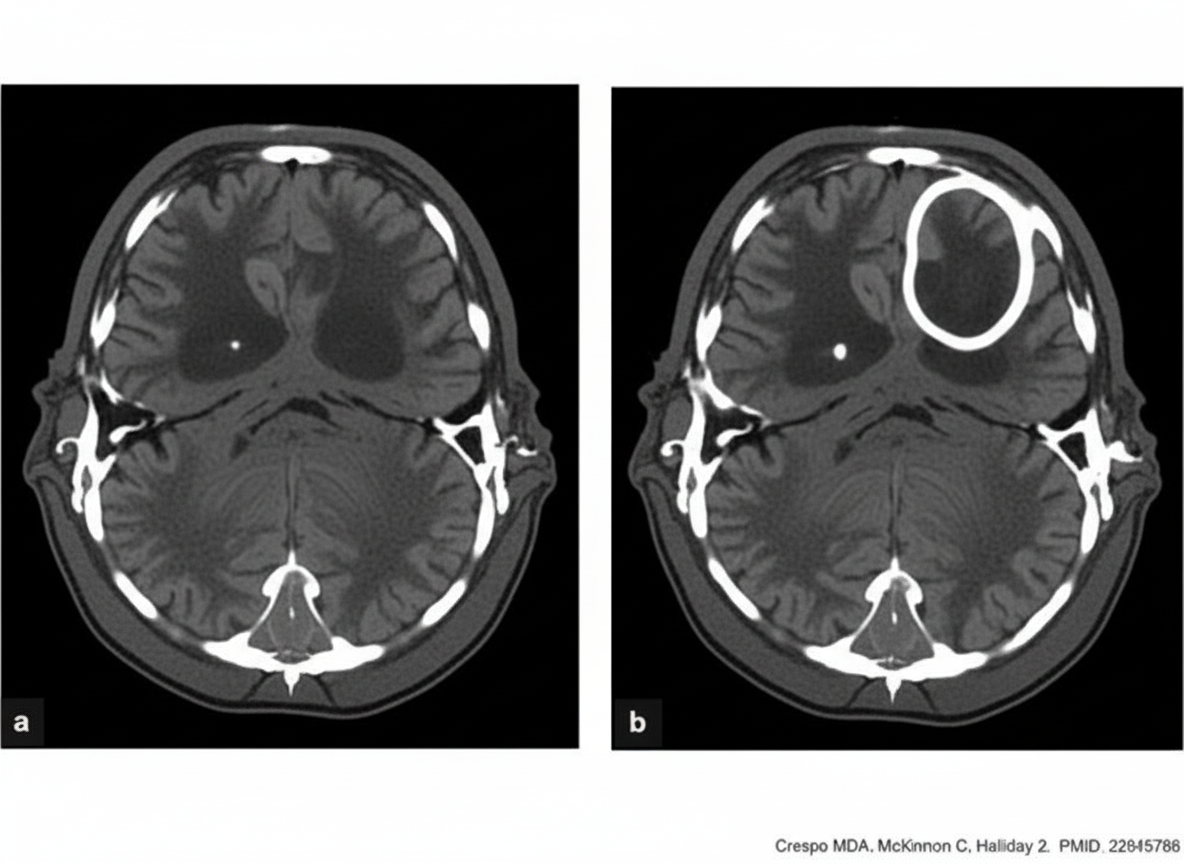
A patient presents with foul-smelling ear discharge and convulsions. What is the appropriate management for this patient, given the CECT findings?
Practice by Chapter
Vestibular System Anatomy and Physiology
Practice Questions
Vestibular Testing
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Neuritis
Practice Questions
Labyrinthitis
Practice Questions
Acoustic Neuroma
Practice Questions
Other Cerebellopontine Angle Tumors
Practice Questions
Facial Nerve Disorders
Practice Questions
Skull Base Surgery
Practice Questions
Cochlear Implantation
Practice Questions
Vestibular Schwannoma Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app