
Neurotology — MCQs

On this page
What is the term for the vertical crest of bone found in the internal acoustic meatus?
Which of the following statements is FALSE regarding acoustic neuroma?
What is true about Vestibular Schwannoma?
Meniere's disease is characterized by all of the following EXCEPT:
Facial nerve palsy is seen in which of the following conditions?
Ramsay Hunt syndrome: all are true EXCEPT?
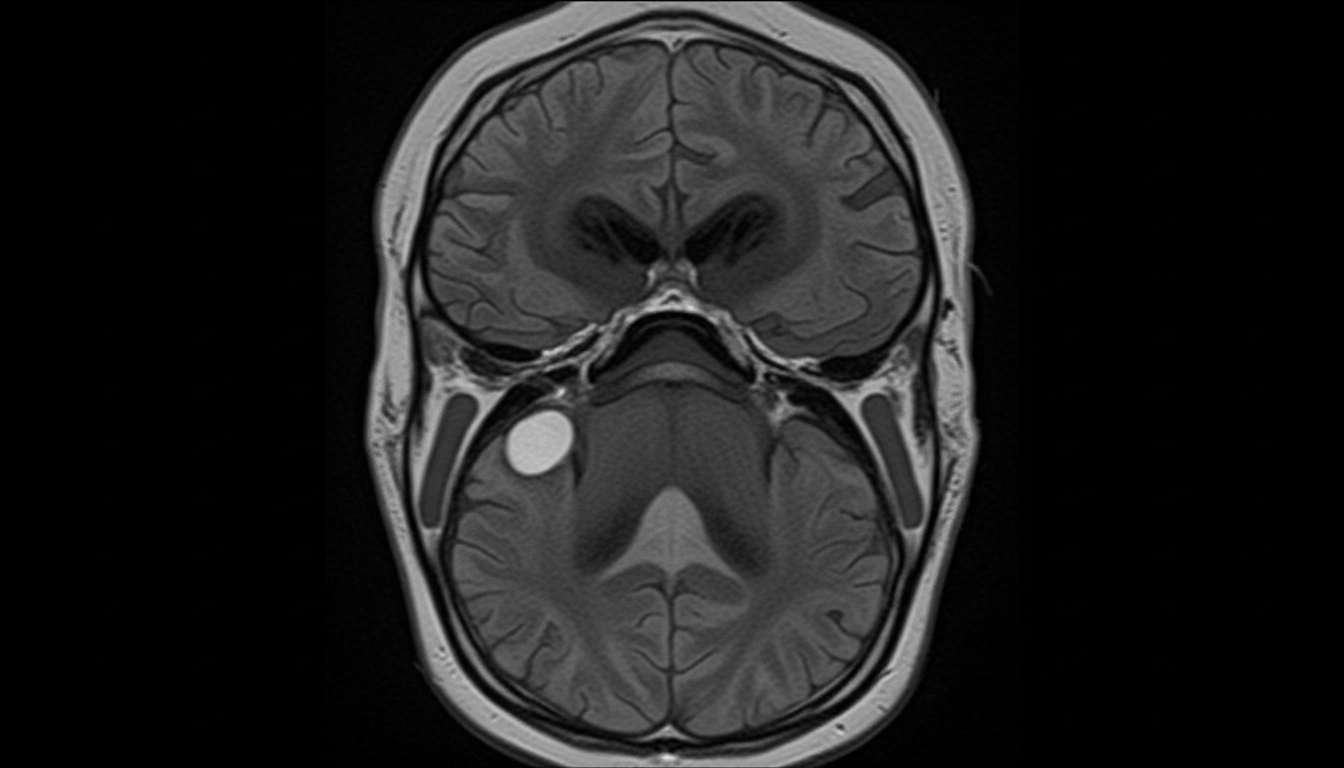
A 50-year-old male presented with progressive unilateral sensorineural hearing loss associated with tinnitus for 2 years. He reported marked difficulty in understanding speech, disproportionate to the pure-tone hearing loss. The patient also complained of reduced corneal sensitivity, numbness, and paresthesia of the face, along with hypoesthesia of the posterior meatal wall. Otoscopy was performed, and audiologic testing revealed a sensorineural type of hearing loss with a poor speech discrimination score, absence of recruitment phenomena, and an SISI score of 0-20%. Based on imaging findings (CEMRI), which of the following structures is LEAST likely to be involved in the most common site for this pathology?
What is the commonest cause of otogenic meningitis?
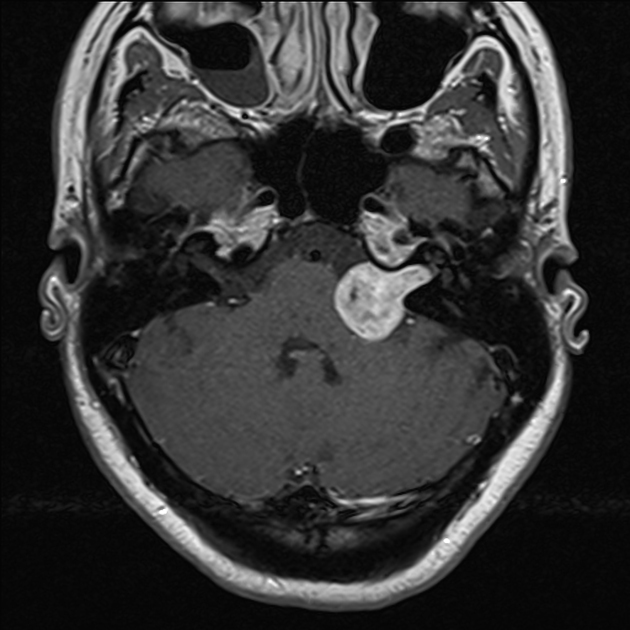
A patient presents with unilateral sensorineural hearing loss and the MRI findings are as shown. What is the most probable diagnosis?
Which of the following is FALSE regarding Gradenigo syndrome?
Practice by Chapter
Vestibular System Anatomy and Physiology
Practice Questions
Vestibular Testing
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Neuritis
Practice Questions
Labyrinthitis
Practice Questions
Acoustic Neuroma
Practice Questions
Other Cerebellopontine Angle Tumors
Practice Questions
Facial Nerve Disorders
Practice Questions
Skull Base Surgery
Practice Questions
Cochlear Implantation
Practice Questions
Vestibular Schwannoma Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app