
Neurotology — MCQs

On this page
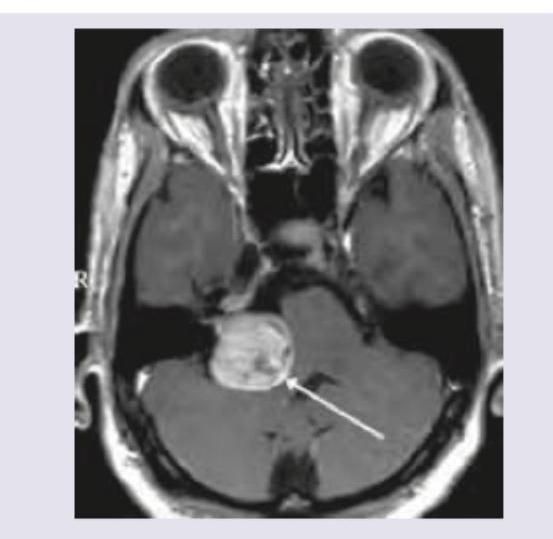
MRI Brain of a 40-year-old patient with progressive unilateral SNHL and tinnitus is shown below. Which is the most commonly affected neighboring cranial nerve after CPA extension of the tumor?
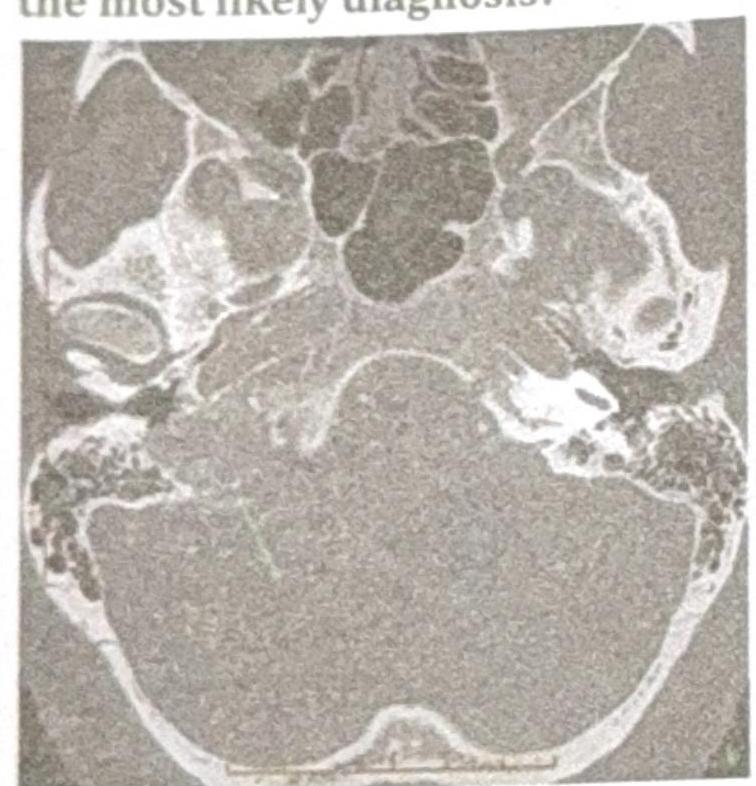
A patient presents with conductive hearing loss, pulsatile tinnitus and a positive Phelps sign. Using the CT scan provided, identify the condition.
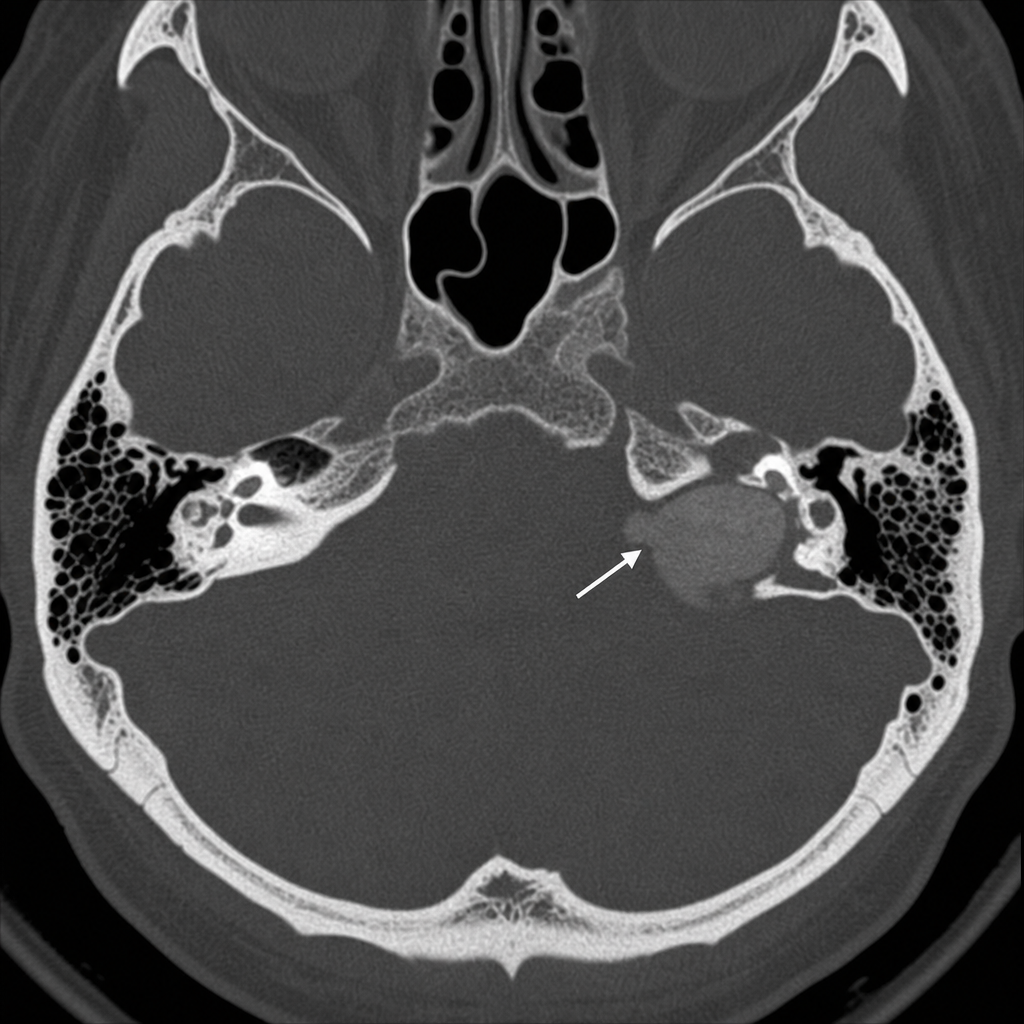
A patient presents with conductive hearing loss, pulsatile tinnitus, and a positive Phelps sign. Based on the CT scan image provided, what is the most likely diagnosis?
The commonest cranial nerve involved in acoustic neuroma is:
Earliest reflex lost in acoustic neuroma -
Which of the following is not true regarding Vestibular neuroma
True about acoustic neuroma:
Acoustic neuroma causes:
All of the following are true about glomus-jugulare tumor except:
If in a patient of acoustic neuroma, corneal reflex is absent it implies involvement of cranial nerve:
Practice by Chapter
Vestibular System Anatomy and Physiology
Practice Questions
Vestibular Testing
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Neuritis
Practice Questions
Labyrinthitis
Practice Questions
Acoustic Neuroma
Practice Questions
Other Cerebellopontine Angle Tumors
Practice Questions
Facial Nerve Disorders
Practice Questions
Skull Base Surgery
Practice Questions
Cochlear Implantation
Practice Questions
Vestibular Schwannoma Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app