
Cochlear Implantation — MCQs

To distinguish between cochlear and post-cochlear damage, which test is done?
Which of the following would be the most appropriate treatment for rehabilitation of a patient, who has bilateral profound deafness following surgery for bilateral acoustic schwannoma?
Arrange the following in the sequence of auditory pathway: 1. Cochlear nucleus 2. Spiral ganglion 3. Superior olivary nucleus 4. Inferior colliculus 5. Medial geniculate body
A child aged 3 yrs, presented with severe sensorineural deafness was prescribed hearing aids, but showed no improvement. What is the next line of management:
Site for placing an electrode in auditory brain stem implant is?
Electrode of cochlear implant is placed in:
Which device is depicted below?
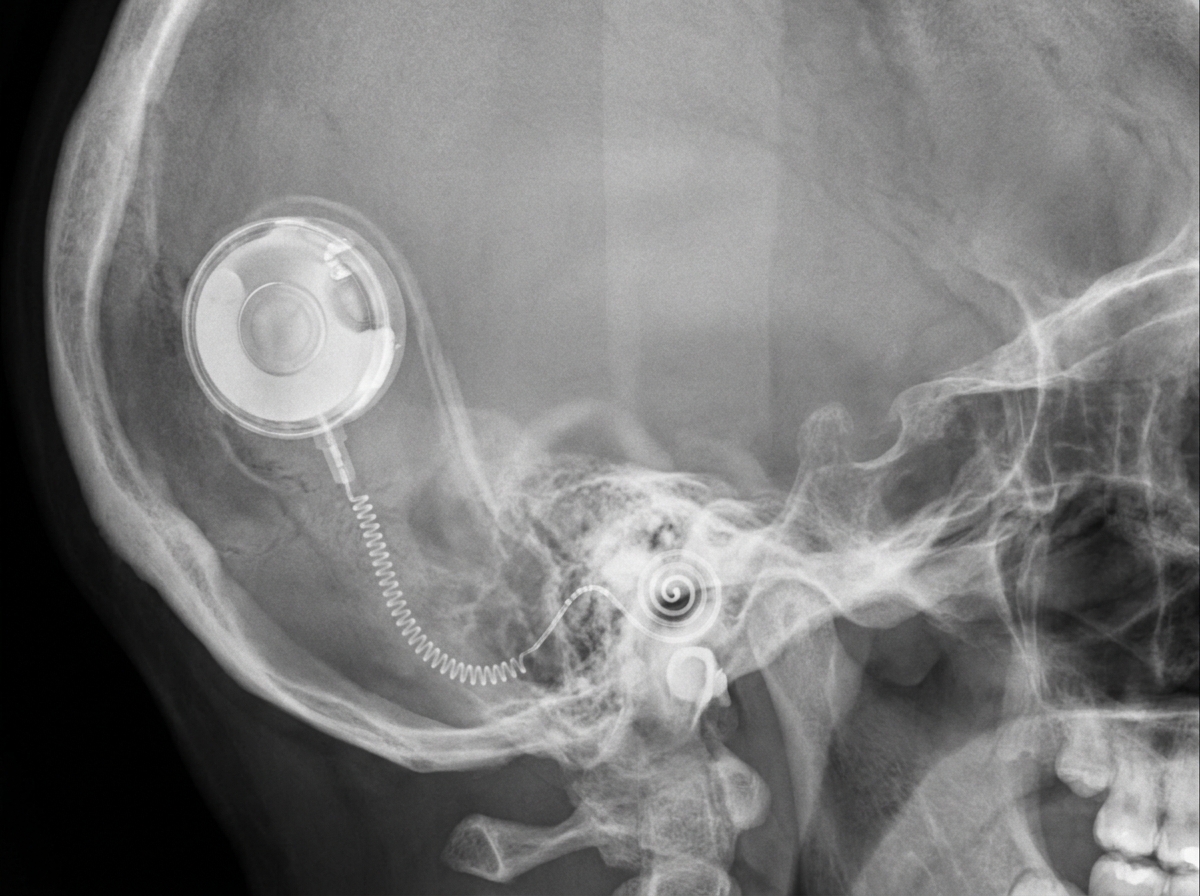
Identify the device shown in the image below:

Which of the following devices typically requires the most stringent safety protocols before MRI scanning?
A 55-year-old man with Bell's palsy for 3 weeks shows no signs of recovery. EMG shows 90% degeneration. Surgical decompression is considered. Which segment of the facial nerve shows maximum compression requiring decompression?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app