
Head and Neck Surgery — MCQs

On this page
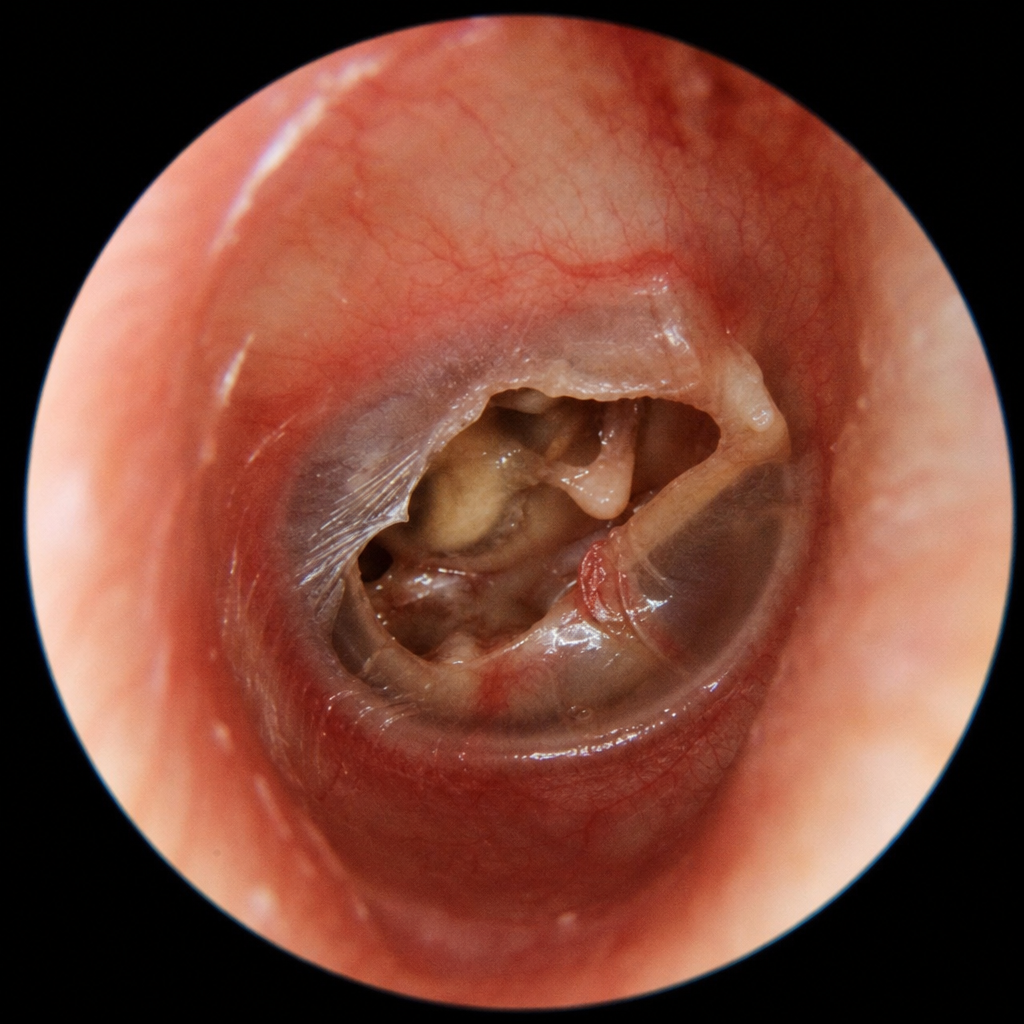
A 38-year-old man presents with a 6-year history of foul-smelling, painless unilateral ear discharge and progressive conductive hearing loss. He denies fever or vertigo. Otoscopy is performed and the image is shown (Image 1). Which of the following best explains the mechanism by which this condition causes progressive hearing loss?
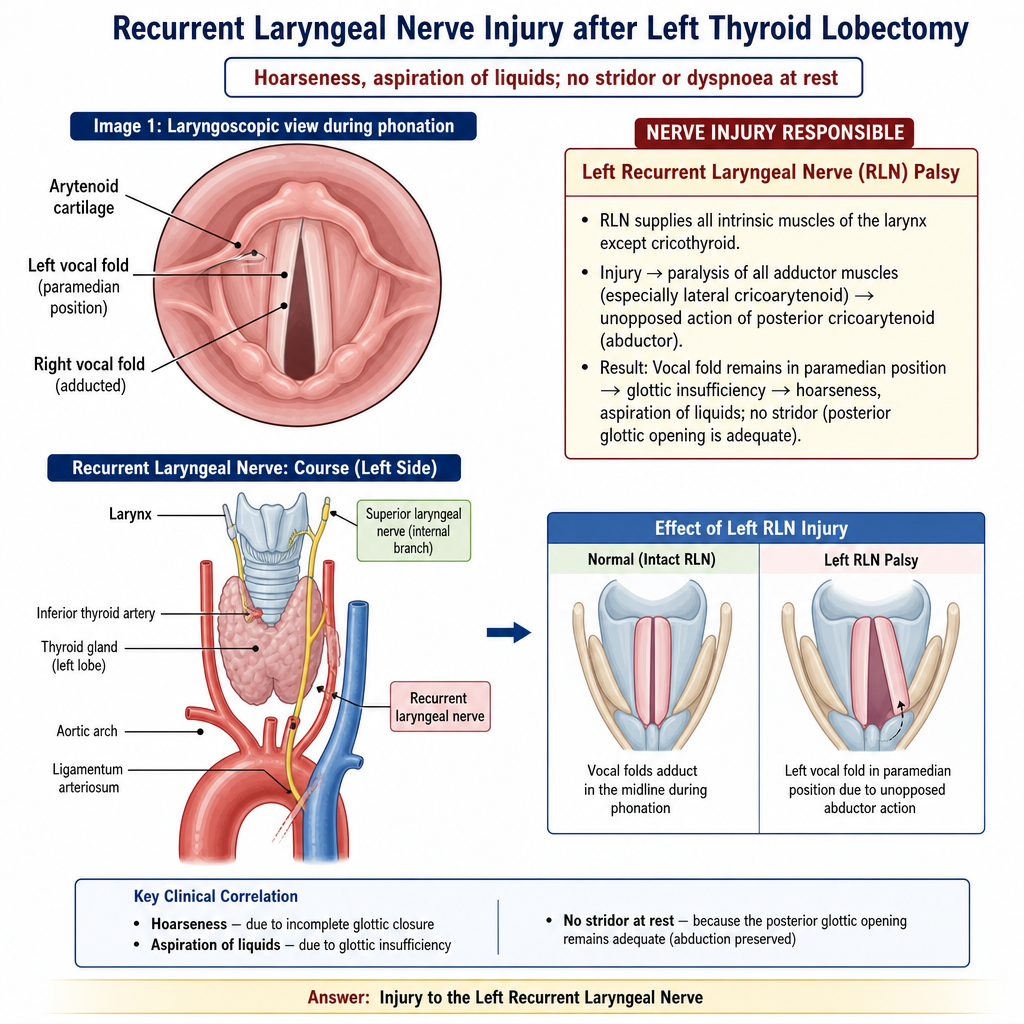
A 58-year-old man presents with a 3-month history of hoarseness and occasional aspiration while drinking liquids following a left-sided thyroid lobectomy. He denies stridor or dyspnoea at rest. His laryngoscopic image taken during phonation is shown (Image 1). Which nerve injury is responsible for the findings seen in this image?
A patient presents with a tumor at the base of the tongue. What is the treatment of choice?
Which structure is damaged in a high tracheostomy?
Secondaries in the neck with no obvious primary malignancy is most often due to which of the following?
Which one of the following is the most common tumor to produce metastasis to cervical lymph nodes?
Which of the following is/are a contraindication for supraglottic laryngectomy?
A 22-year-old woman underwent tracheostomy during hospitalization following a major motor vehicle accident. Five days post-tracheostomy, she develops minor bleeding around the site. What is the most appropriate immediate management?
Which of the following statements regarding branchial anomalies is true?
Which of the following comprises Level V cervical nodes?
Practice by Chapter
Neck Spaces and Fasciae
Practice Questions
Congenital Neck Lesions
Practice Questions
Neck Masses: Differential Diagnosis
Practice Questions
Thyroid Nodules and Cancer
Practice Questions
Parathyroid Disorders
Practice Questions
Cervical Lymphadenopathy
Practice Questions
Neck Dissection Principles
Practice Questions
Deep Neck Space Infections
Practice Questions
Carotid Body Tumors
Practice Questions
Reconstruction Principles in Head and Neck
Practice Questions
Management of Head and Neck Cancer
Practice Questions
Complications in Head and Neck Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app