
Nasal Reconstruction — MCQs

One of the most important complication of tracheostomy is:
A nasal surgery was carried out with the incision shown in the image. What was the procedure likely carried out?

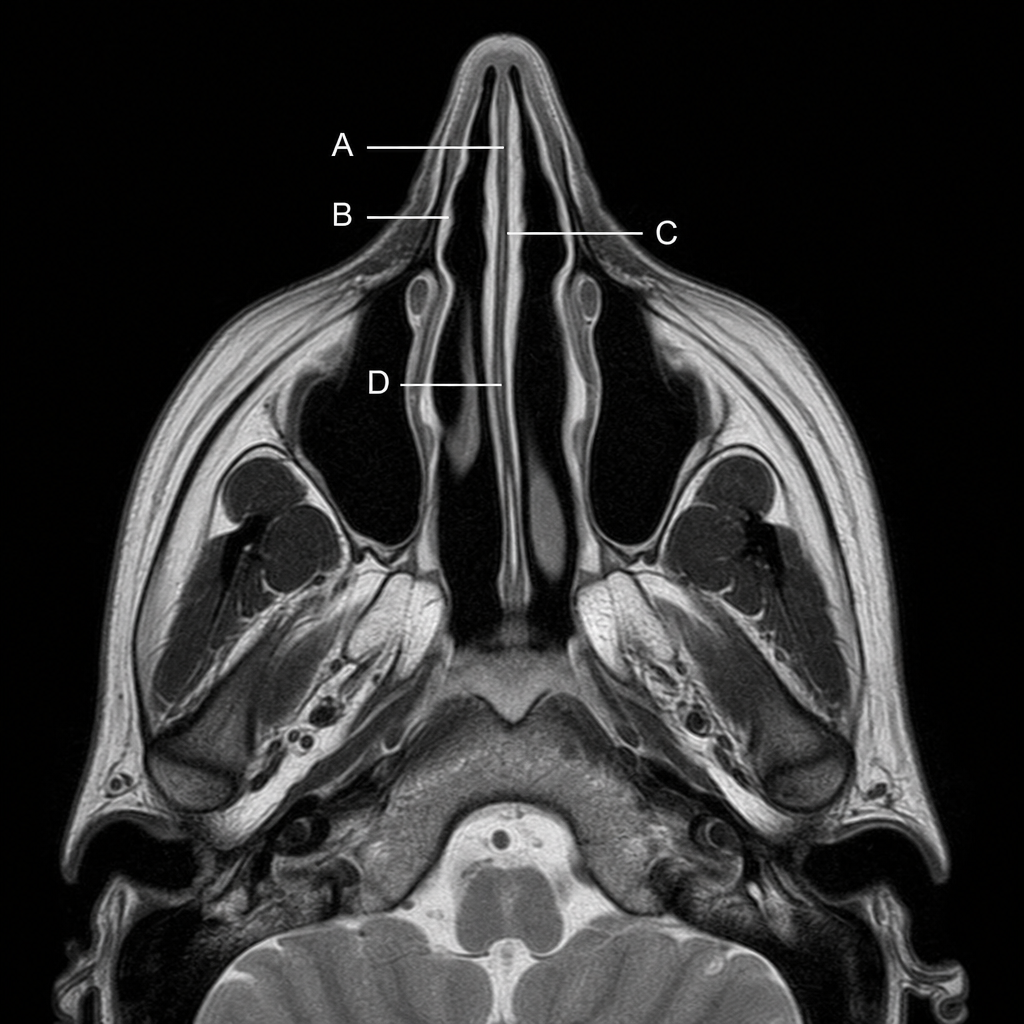
Choose the appropriate lettered structure in this MRI scan showing a transaxial section through the head. Which structure is formed by the perpendicular plate of the ethmoid bone, vomer, and septal cartilage?
In which of the following situations is breast conservation surgery not indicated?
What is the eponymous term for a full-thickness skin graft?
Which flap is commonly used in breast reconstruction?
Where is a nasal antrostomy typically created following a Caldwell-Luc procedure?
Which of the following arteries is a branch of the facial artery?
In which condition is Young's operation performed?
Atrophic dry nasal mucosa, extensive encrustations, and a woody hard external nose are most suggestive of:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app