
Cleft Lip and Palate Repair — MCQs

Which index is used to score the outcome of treatment in patients with cleft lip and palate?
A patient complains of loss of visual acuity, deafness, and enlargement of the maxilla.

Millard repair is used for treatment of:
Hynes pharyngoplasty is used to improve a child's?
What is the primary challenge in constructing a complete denture for a patient with Bell's palsy?
A midline cleft lip results from failure of fusion between which structures?
Repair of cleft lip should be undertaken at:
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Unilateral cleft lip is repaired at what age?
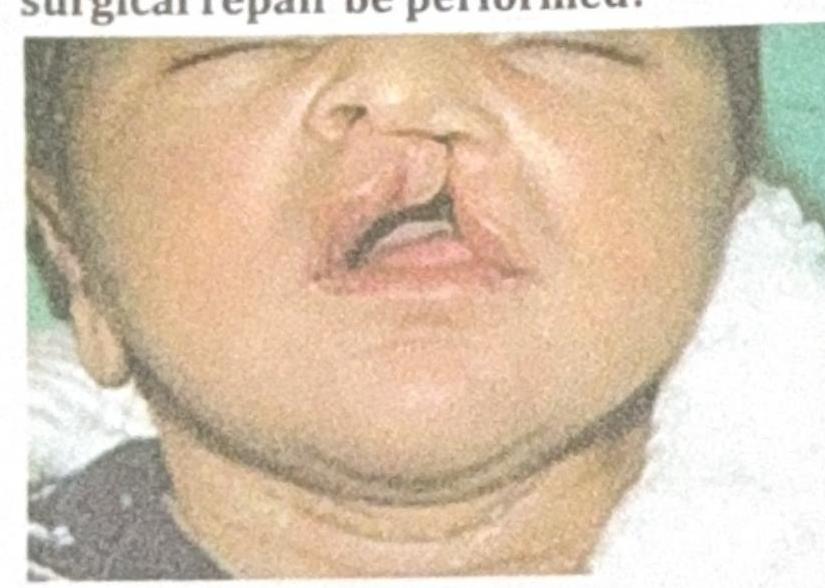
A child presents to the OPD with the finding shown in the image. When should the first surgical repair be performed?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app