
Retropharyngeal Abscess — MCQs

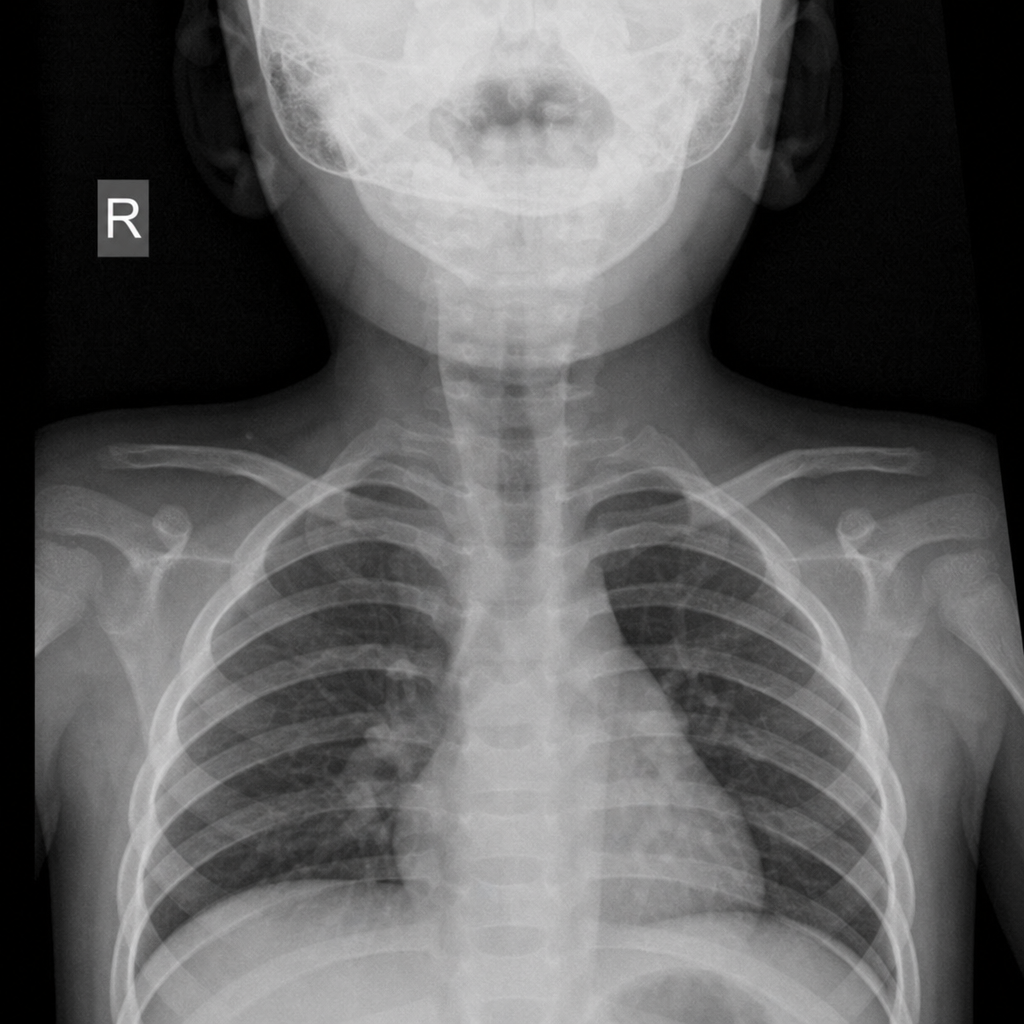
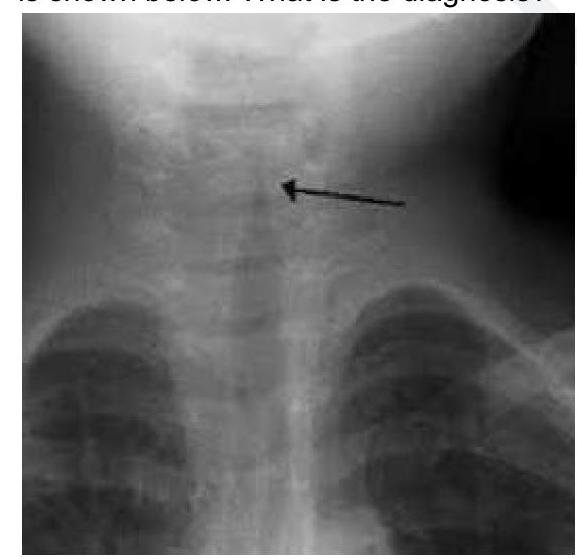
A 2-year-old child presented with the following x-ray finding. What is the most likely diagnosis?
Not true about parapharyngeal abscess?
What is the most appropriate antibiotic choice for a 4-year-old unvaccinated child with epiglottitis?
A 25-year-old woman presents with severe throat pain, difficulty swallowing, and trismus. CT neck shows a peritonsillar fluid collection and inflammation. What is the next best step?
A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
Which of the following statements about acute retropharyngeal abscess is true?
A patient presented with 2 days history of fever. On examination there was a swelling in the neck and one side tonsil was pushed to midline. What is the most likely diagnosis:-
A 15 years old Male presented with history of fever since 2 days, unable to swallow the food with muffled voice. On examination it is noted right tonsil is shifted to midline. What is the diagnosis:
Trismus in parapharyngeal abscess is caused by spasm of which of the following muscles?
Early tonsillectomy is not done in?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app