
Acute Laryngitis — MCQs

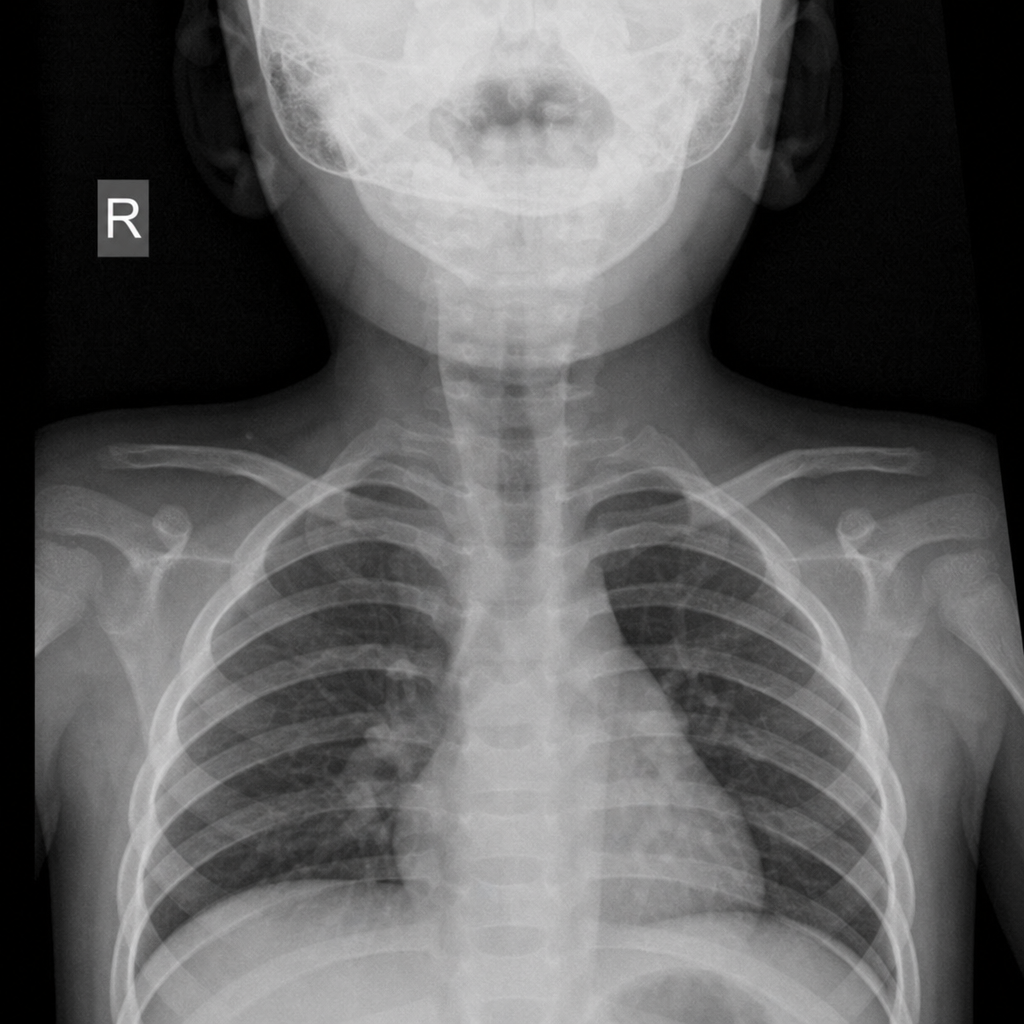
A 2-year-old child presented with the following x-ray finding. What is the most likely diagnosis?
To prevent acute rheumatic fever, acute pharyngitis due to group A streptococci should be treated with antibiotics before:
A 50-year-old smoker presents with hoarseness, dysphagia, and weight loss. Flexible laryngoscopy shows a mass on the vocal cords. What is the next best step?
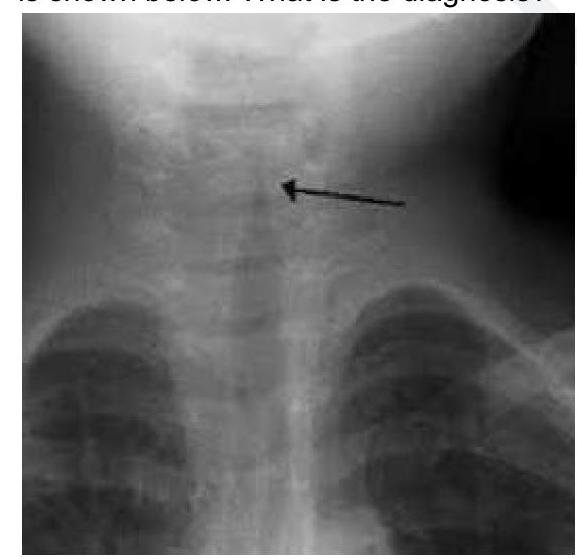
A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
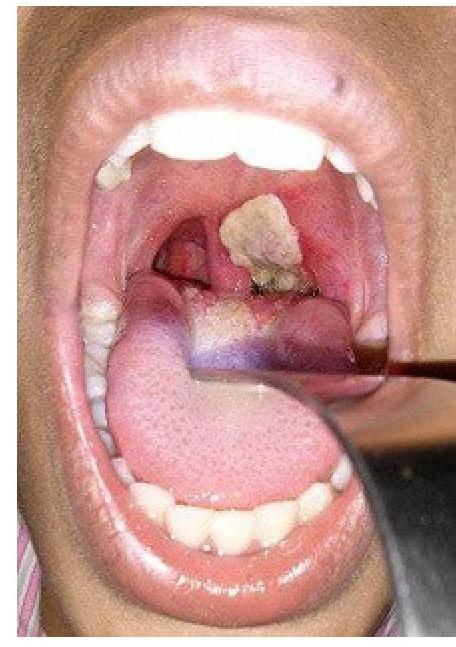
A child presents with high grade fever, inspiratory stridor and develops swallowing difficulty with drooling of saliva since last 4-6 hours. Which of the following treatment is recommended apart from general airway management?
A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
Laryngitis sicca is associated with ?
Inspiratory stridor is due to lesions of:
Killian's Dehiscence is seen at the level of:
A 58-year-old man, chronic smoker, presents with progressive hoarseness of voice and throat discomfort for 4 months. Laryngoscopy reveals a laryngeal growth, and neck examination shows a single ipsilateral, mobile cervical lymph node. Biopsy confirms squamous cell carcinoma of the larynx. What is the most appropriate treatment?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app