
Sudden Sensorineural Hearing Loss — MCQs

A 25-year-old woman presents with episodes of dizziness, tinnitus, and hearing loss in the right ear. What is the most likely diagnosis?
In a patient with acoustic neuroma all are seen except:
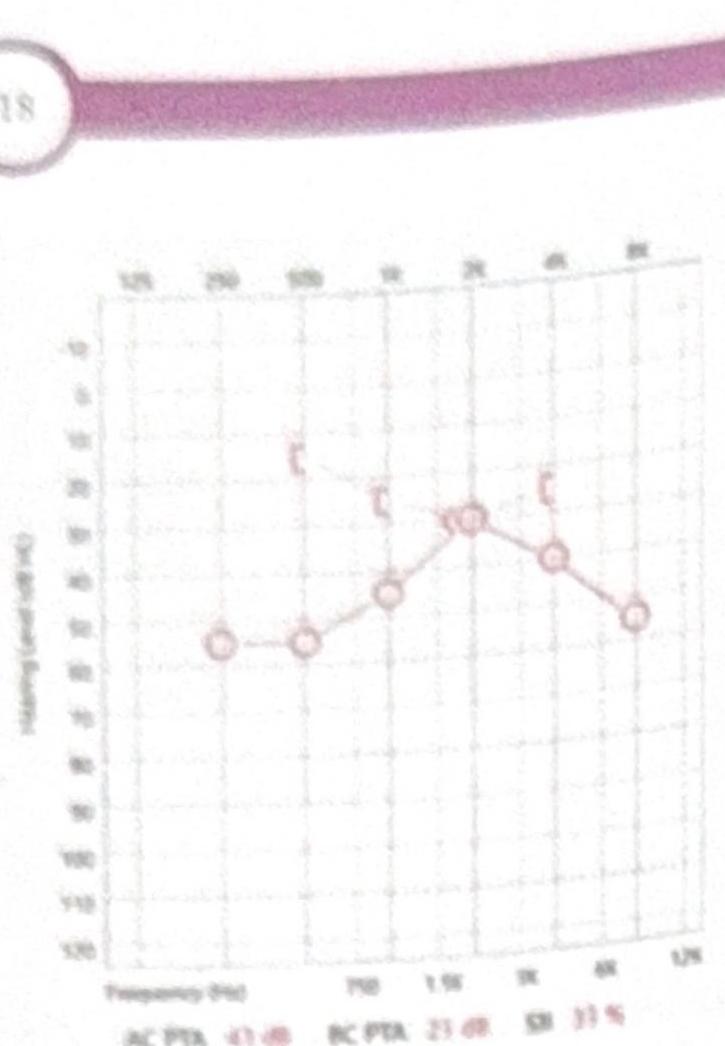
A female patient presents with mild conductive hearing loss (CHL) and tinnitus. Based on the pure tone audiometry (PTA) shown in the image, what is the most likely diagnosis?
A child aged 3 yrs, presented with severe sensorineural deafness was prescribed hearing aids, but showed no improvement. What is the next line of management:
35 years old female presents with tinnitus, vertigo and aural fullness. Likely diagnosis:
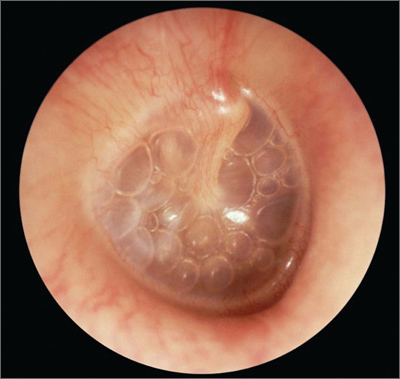
A 5-year-old child presents with reduced hearing for the past 2-3 months. Based on the otoscopy findings shown, what is the most likely diagnosis?
Most common cause of sensorineural hearing loss (SNHL)
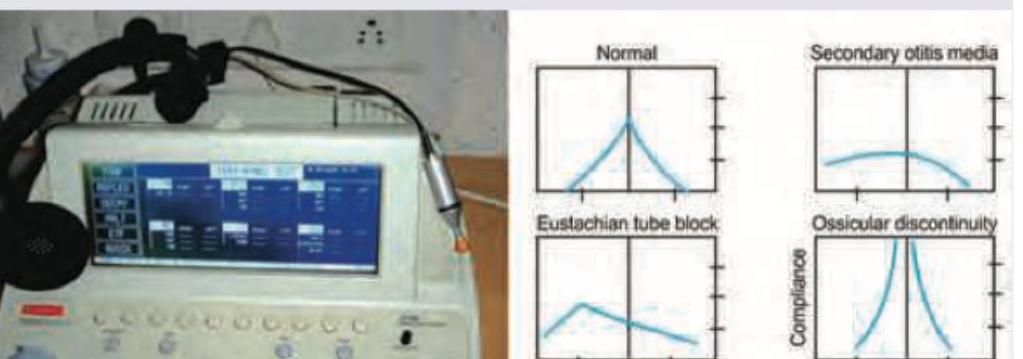
A patient presents with fullness in the ear and hearing loss. Tympanometry shows a type B curve. What does this indicate?
The following test is useful for diagnosis of all except:
A 72-year-old man presents to his primary care physician with progressively worsening hearing loss. He states that his trouble with hearing began approximately 7-8 years ago. He is able to hear when someone is speaking to him; however, he has difficulty with understanding what is being said, especially when there is background noise. In addition to his current symptoms, he reports a steady ringing in both ears, and at times experiences dizziness. Medical history is significant for three prior episodes of acute otitis media. Family history is notable for his father being diagnosed with cholesteatoma. His temperature is 98.6°F (37°C), blood pressure is 138/88 mmHg, pulse is 74/min, and respirations are 13/min. On physical exam, when a tuning fork is placed in the middle of the patient's forehead, sound is appreciated equally on both ears. When a tuning fork is placed by the external auditory canal and subsequently on the mastoid process, air conduction is greater than bone conduction. Which of the following is most likely the cause of this patient's symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app