
Diseases of the Ear — MCQs

On this page
Which of the following best describes glue ear?
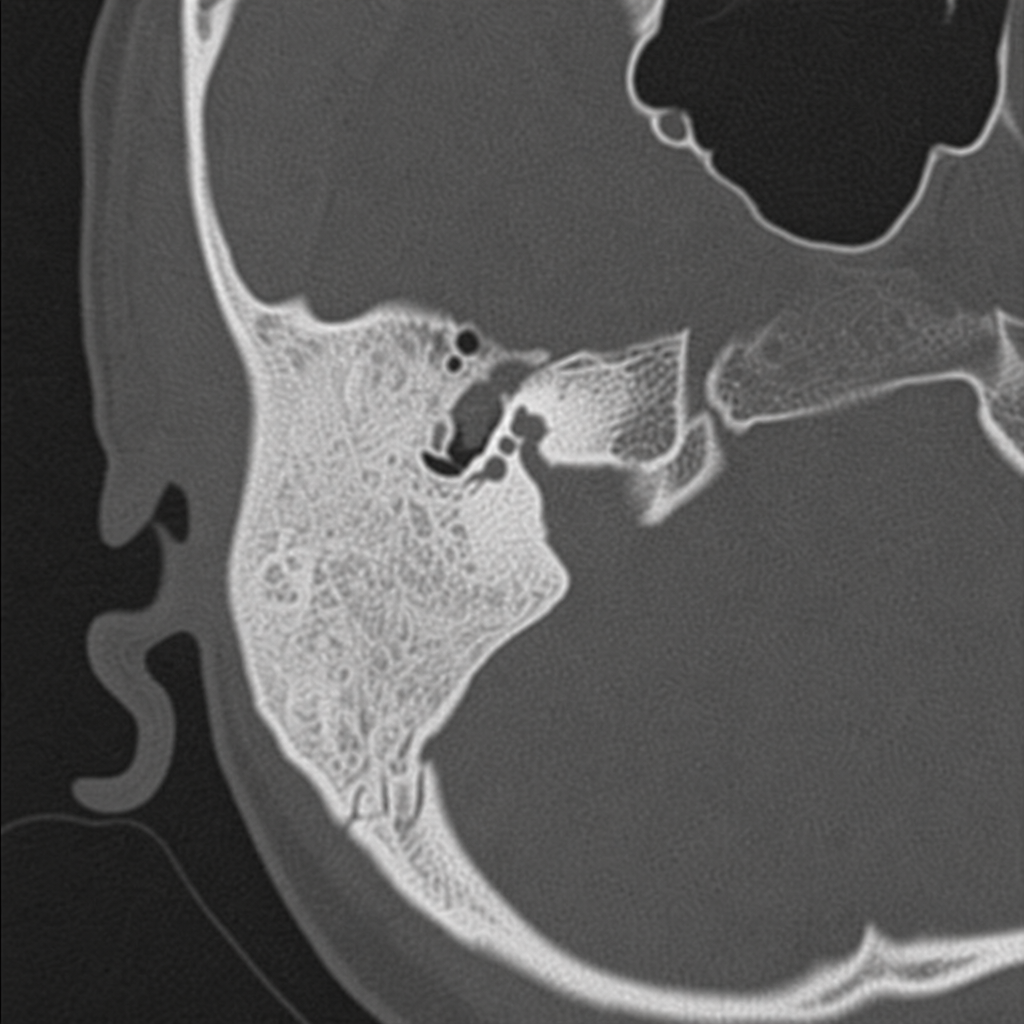
An axial CT scan of the mastoid is shown below. Which type of mastoid pneumatization is depicted among the given options?
Which nerve is responsible for referred pain in the ear?
What is the treatment of choice for unsafe CSOM with cholesteatoma and sensorineural deafness?
Referred otalgia can be due to which of the following?
A 5-year-old child has had eight episodes of acute otitis media in 6 months and has difficulty resolving the effusions between infections. What is the most effective management strategy?
Mastoid infection which erodes through the outer cortex of bone results in what?
A patient with facial nerve paralysis suffers from inability to dampen loud noises due to denervation of which muscle?
Which of the following is NOT true about hearing loss in otosclerosis?
What is the treatment of choice in central perforation?
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app