
Diseases of the Ear — MCQs

On this page
What is the primary treatment for attico-antral disease?
Which cranial nerve is most commonly damaged in Chronic Suppurative Otitis Media (CSOM)?
A 5-year-old child presents with reduced hearing for the past 2-3 months. Based on the otoscopy findings shown, what is the most likely diagnosis?
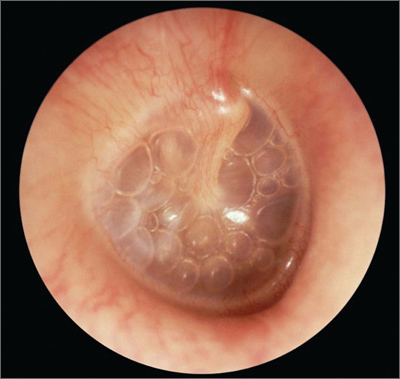
Which diagnosis is most consistent with this otoscopic image?
Which of the following is NOT a characteristic of Tubercular Otitis Media?
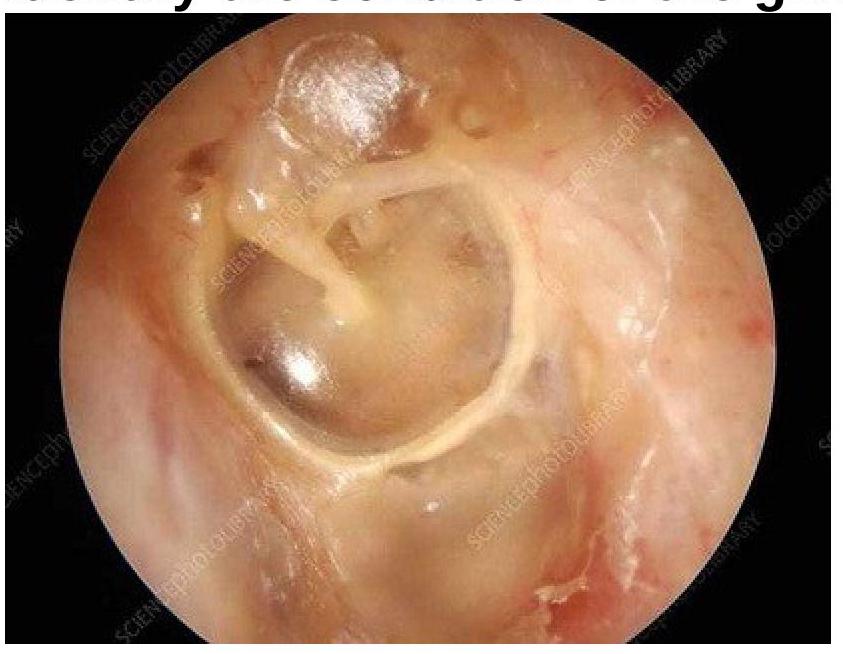
A patient presented with painless chronic otorrhea, a history of tuberculosis exposure, and a positive mycobacterial culture. The following picture of the Tympanic Membrane was obtained. What is the most probable diagnosis (marked with arrow)?

Which perforation of the tympanic membrane is most commonly seen with tubotympanic CSOM?
All of the following are features of Tubotympanic CSOM except which of the following?
Most common cause of otitis externa is
Otosclerosis affects which bone?
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app