
Diseases of the Ear — MCQs

On this page
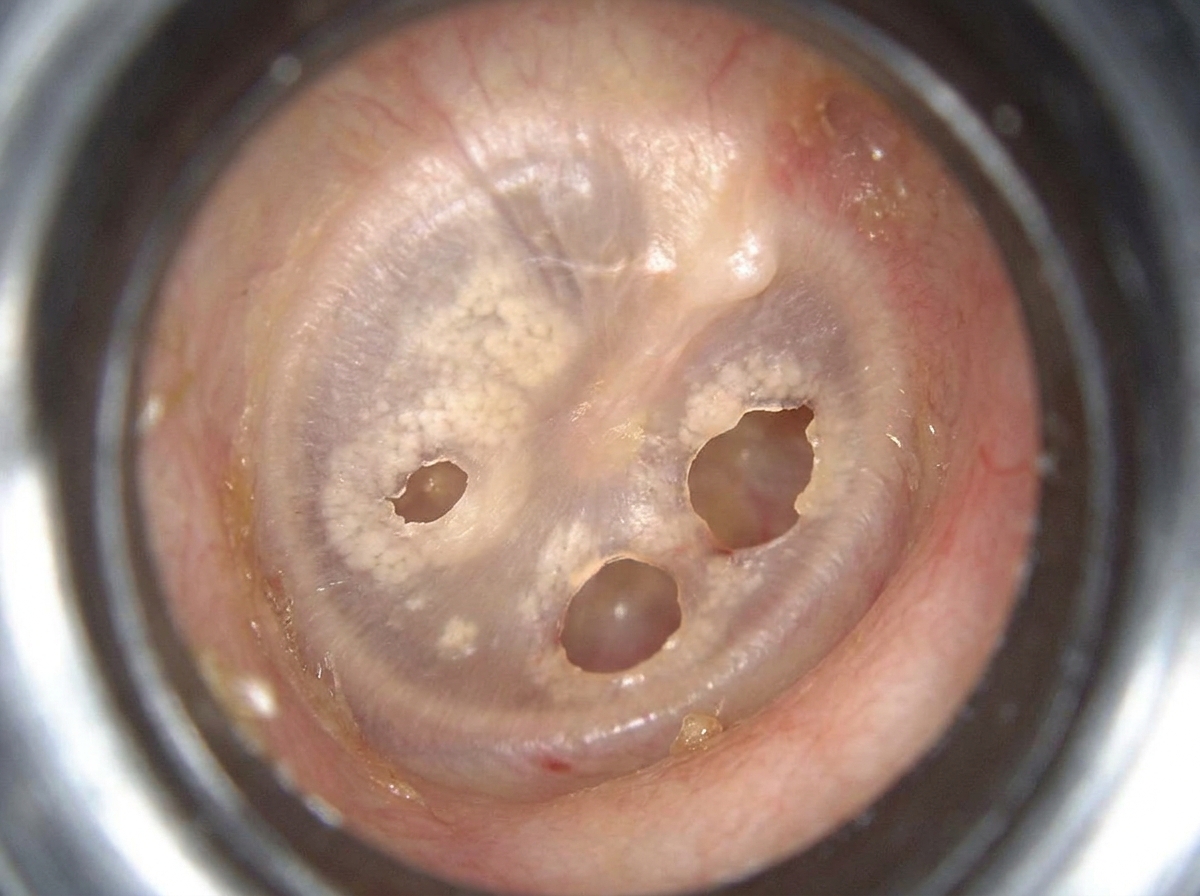
A patient presented with the following picture of Tympanic Membrane. Most Probable diagnosis:
Which of the following is not a direct treatment option for central safe perforation of the tympanic membrane?
All of the following are true about malignant otitis externa except which of the following?
Which of the following statements about serous otitis media is false?
Which ossicle is most commonly involved in CSOM?
Most common malignancy of middle ear is
A 10 year old child presents with painless, non-foul-smelling purulent discharge from the ear. Patient reports that he is able to hear better in the presence of discharge than when the ear is dry. The most probable diagnosis is
A diabetic patient presents with foul smelling ear discharge, fever and severe pain in the ear. On examination there is thick yellow coloured discharge from the ear and granulation tissue in the canal. Which of the following is the appropriate management for this patient?
Which of the following is included in the Levenson criteria for congenital cholesteatoma?
What condition is characterized by multiple perforations of the tympanic membrane?
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app