
Diseases of the Ear — MCQs

On this page
In a patient with unilateral hearing loss and tinnitus, which anatomical part of the ear is likely to be affected?
A patient presents with a history of recurrent otitis media and a tympanic membrane perforation. What is the most common complication?
A 25-year-old swimmer presents with ear pain and discharge. Otoscopy reveals inflammation of the external ear canal. What is the most likely diagnosis?
Otosclerosis is inherited in which manner?
A 4-year-old child presents with difficulty hearing and frequent ear infections. An otoscopic examination reveals fluid in the middle ear without signs of acute infection. What is the most likely diagnosis?
A 60-year-old male presents with unilateral conductive hearing loss and a pearly white mass behind the tympanic membrane. What is the most likely diagnosis?
A 4-year-old child presents with a history of recurrent ear infections, poor school performance, and behavioral problems. Audiometry confirms bilateral conductive hearing loss. What is the most likely diagnosis?
A 3-year-old child presents with severe otalgia, fever of 39.5°C for 2 days, and bulging tympanic membrane. What is the primary treatment for this acute otitis media?
A 35-year-old patient presents with recurrent otitis media. Tympanometry reveals a type B tympanogram. What is the best management option?
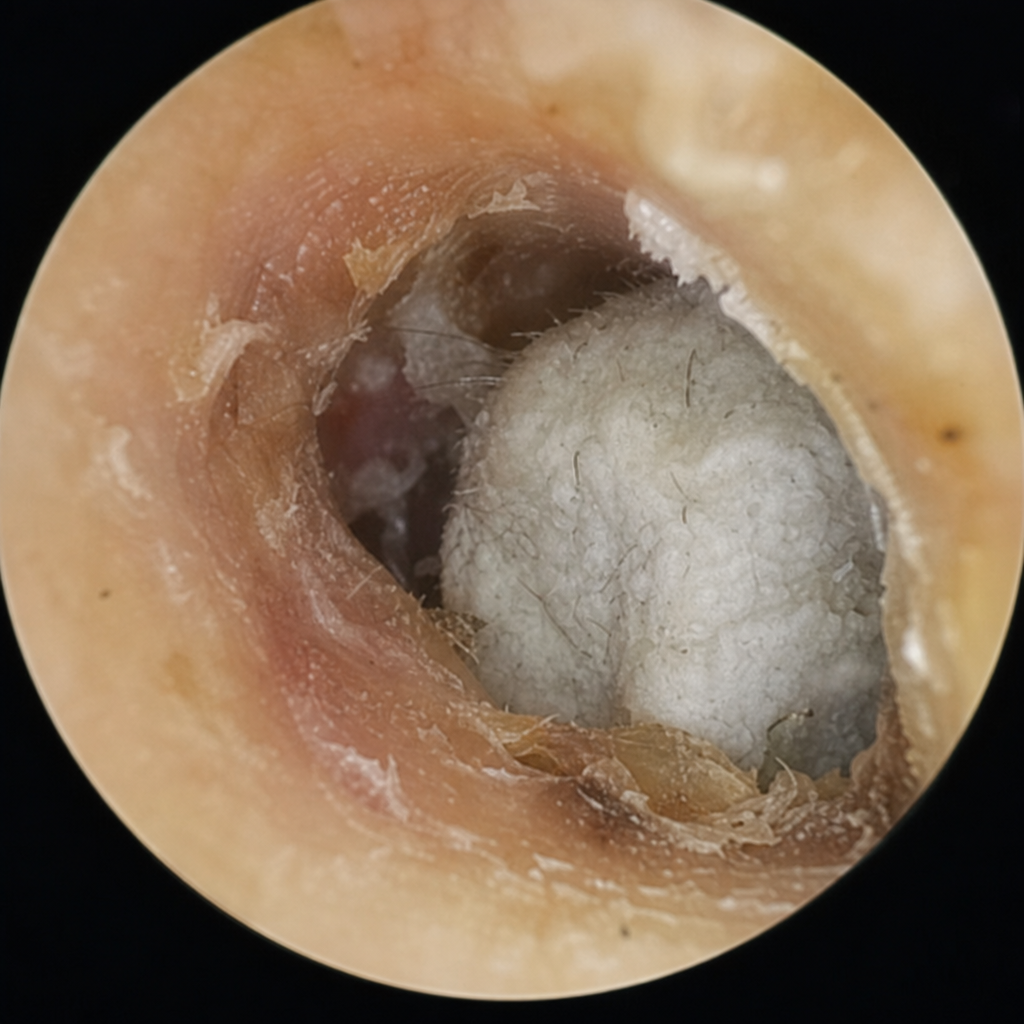
Identify the condition based on the provided image.
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app