
Diseases of the Ear — MCQs

On this page
A patient presents with ear discharge. The CT image is shown below. Based on the clinical presentation and imaging, what is the most likely diagnosis?
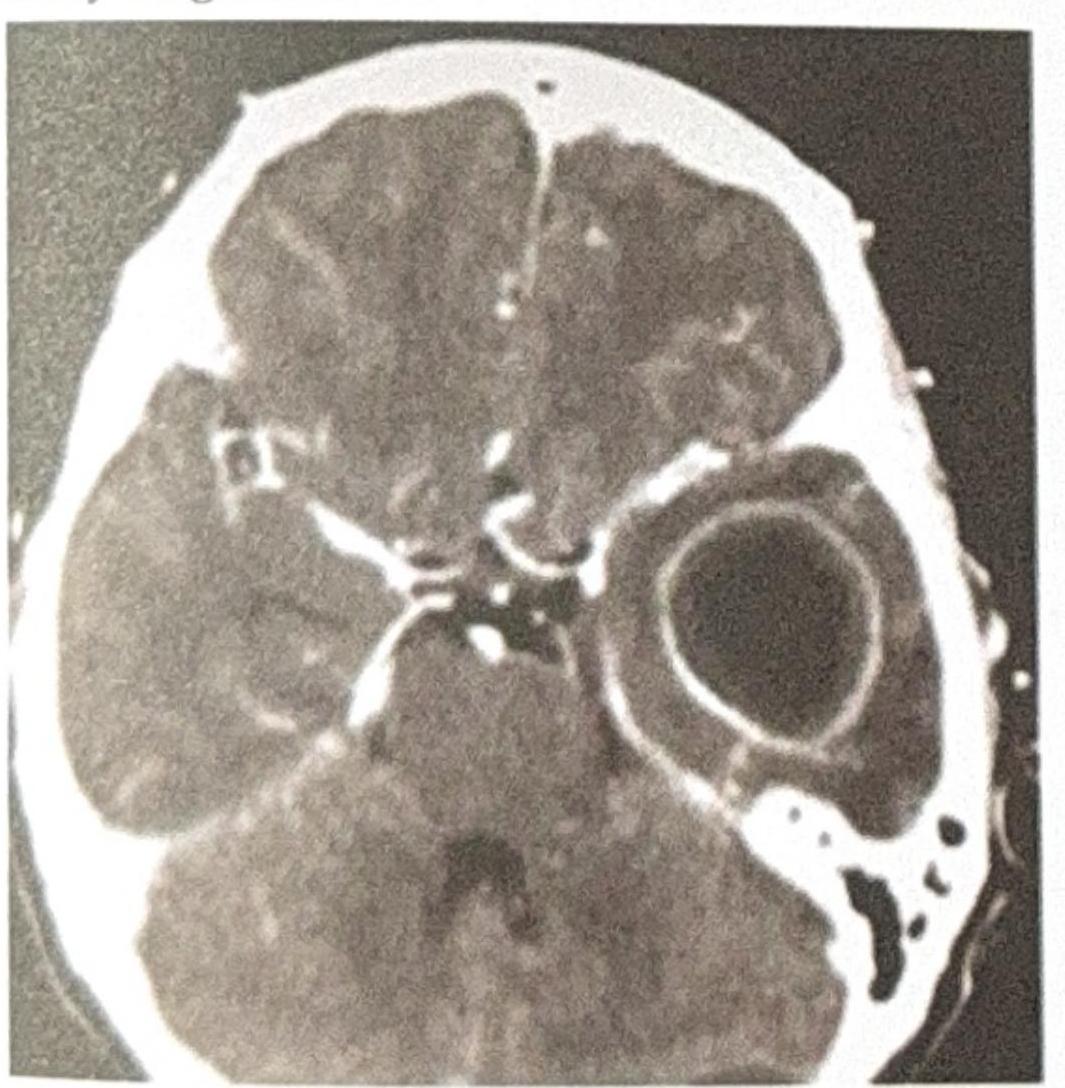
A patient with a history of chronic ear infection now presents with manifestations, including headache and vomiting. A CT brain image is shown. What is the most probable diagnosis?

A 72-year-old man presents to his primary care physician with progressively worsening hearing loss. He states that his trouble with hearing began approximately 7-8 years ago. He is able to hear when someone is speaking to him; however, he has difficulty with understanding what is being said, especially when there is background noise. In addition to his current symptoms, he reports a steady ringing in both ears, and at times experiences dizziness. Medical history is significant for three prior episodes of acute otitis media. Family history is notable for his father being diagnosed with cholesteatoma. His temperature is 98.6°F (37°C), blood pressure is 138/88 mmHg, pulse is 74/min, and respirations are 13/min. On physical exam, when a tuning fork is placed in the middle of the patient's forehead, sound is appreciated equally on both ears. When a tuning fork is placed by the external auditory canal and subsequently on the mastoid process, air conduction is greater than bone conduction. Which of the following is most likely the cause of this patient's symptoms?
Mainstay of treatment of glue ear -
Most common cause of sensorineural hearing loss (SNHL)
Cold water is not used for ear cleaning because
Tobey-Ayer test is done for:
Most common cause of facial nerve palsy:
Most common cause of syndromic deafness is:
Gelle's test is for:
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app