
Diseases of the Ear — MCQs

On this page
What does the following image show?
What does the following image show?

All are true about the lesion marked except:
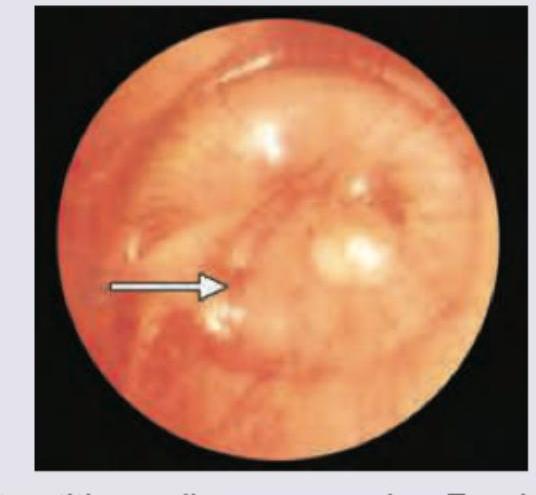
A 1-year-old child presents with high grade fever for 2 days with multiple episodes of loose motions. The child is inconsolable. The otoscopic finding is given below. All of the following lead to the development of this condition except:
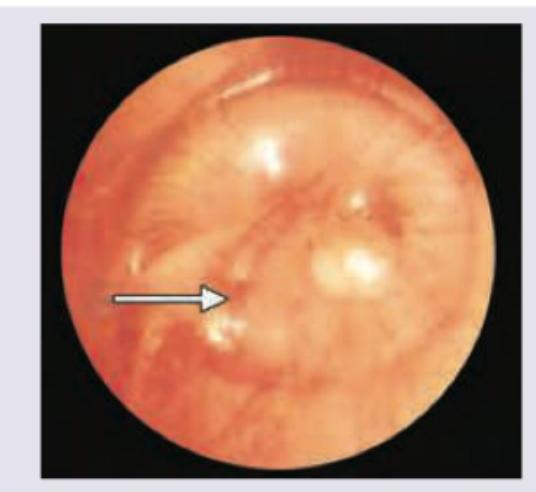
A 1-year-old child presents with high grade fever for 2 days with multiple episodes of loose motions. The child is inconsolable. The otoscopic finding is given below. What is the diagnosis?
Which of the following is correct about ear speculum insertion?
A 2-year-old child presents with profuse odorless ear discharge for the past 6 weeks following a URTI. Otoscopic examination shows:

What is the diagnosis shown in the following image?
Which one of the following conditions produces sensorineural deafness ?
A female patient aged 30 years with bilateral conductive deafness is wearing a hearing aid. What is the probable diagnosis?
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app