
Noise-Induced Hearing Loss — MCQs

Tests of SNHL are characterized by all EXCEPT
A pure tone audiogram showing a bone conduction dip (Carhart notch) at 2000 Hz is characteristic of-
What is the maximum allowable noise exposure according to the Indian Factory Act?
The acceptable noise level that can be tolerated without any damage to hearing is:
All the following are true about Meniere's disease except?
35 years old female presents with tinnitus, vertigo and aural fullness. Likely diagnosis:
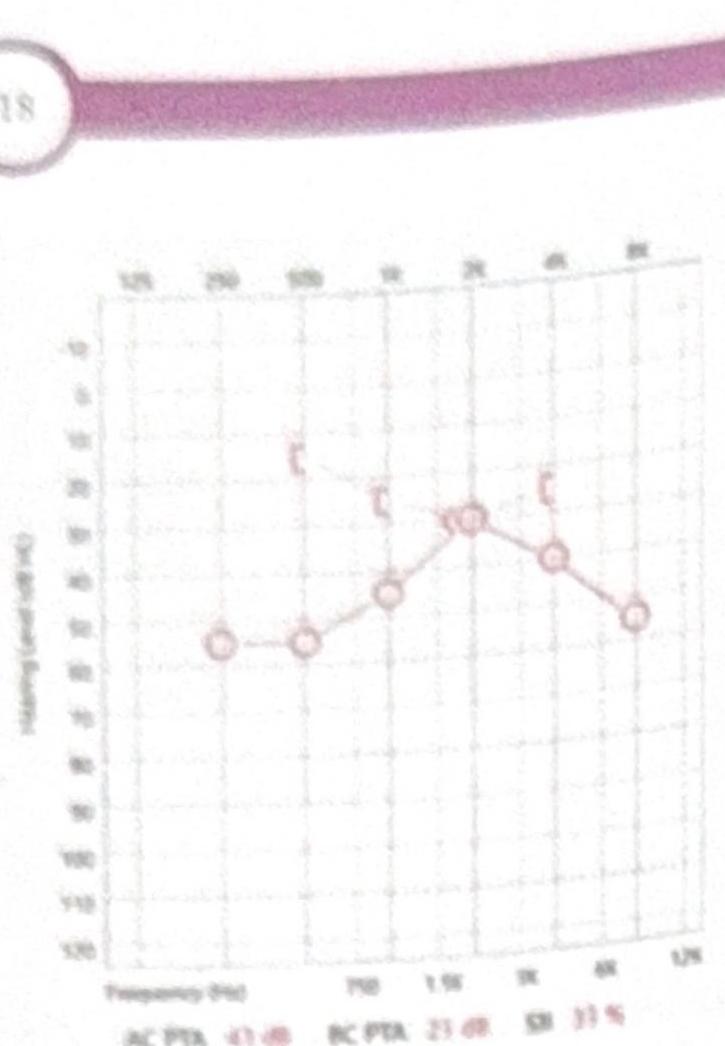
A female patient presents with mild conductive hearing loss (CHL) and tinnitus. Based on the pure tone audiometry (PTA) shown in the image, what is the most likely diagnosis?
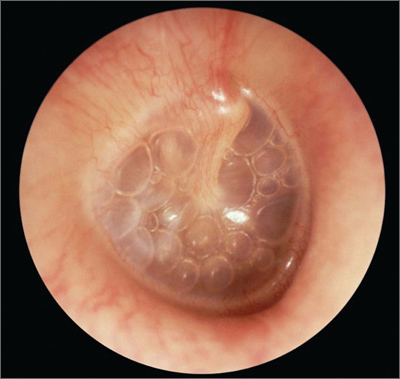
A 5-year-old child presents with reduced hearing for the past 2-3 months. Based on the otoscopy findings shown, what is the most likely diagnosis?
A patient presents with fullness in the ear and hearing loss. Tympanometry shows a type B curve. What does this indicate?
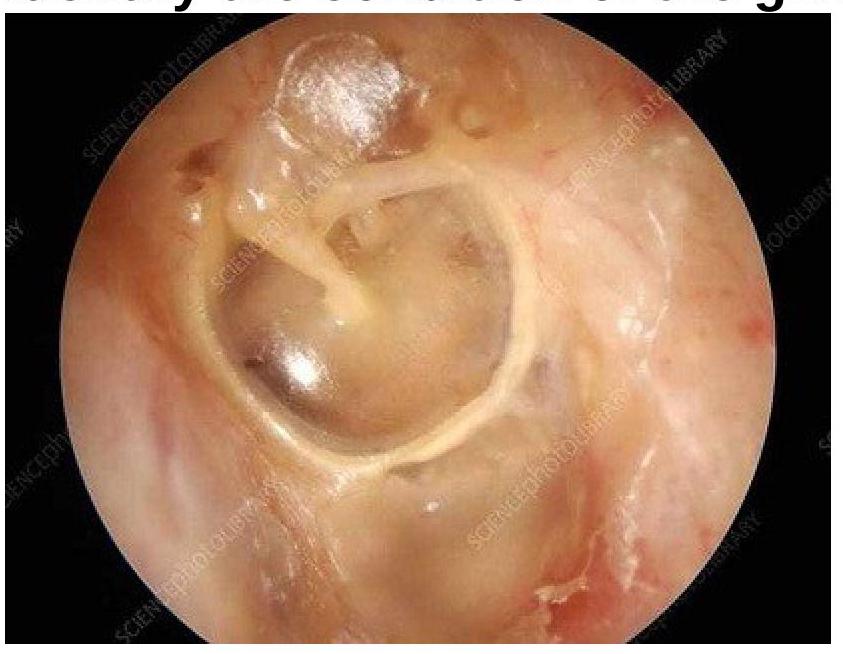
Identify the condition of the given image:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app