
Diseases of the Ear — MCQs

On this page
A 40 year old presented with bilateral hearing loss. Audiogram shows a dip at 2000 Hz. What is the most appropriate investigation?
A factory worker presents with bilateral hearing difficulty. Audiometry is as shown in the image. This pattern is characteristic of:
A 35-year-old patient presents with hearing loss. Clinical examination reveals a Rinne test where Air Conduction is greater than Bone Conduction in both ears. The Weber test lateralizes to the left ear. What is the most likely diagnosis?
A patient develops acute-onset severe unilateral hearing loss with no identifiable cause. Audiometry confirms sensorineural hearing loss. Which of the following pharmacological regimens is considered the first-line treatment for this condition?
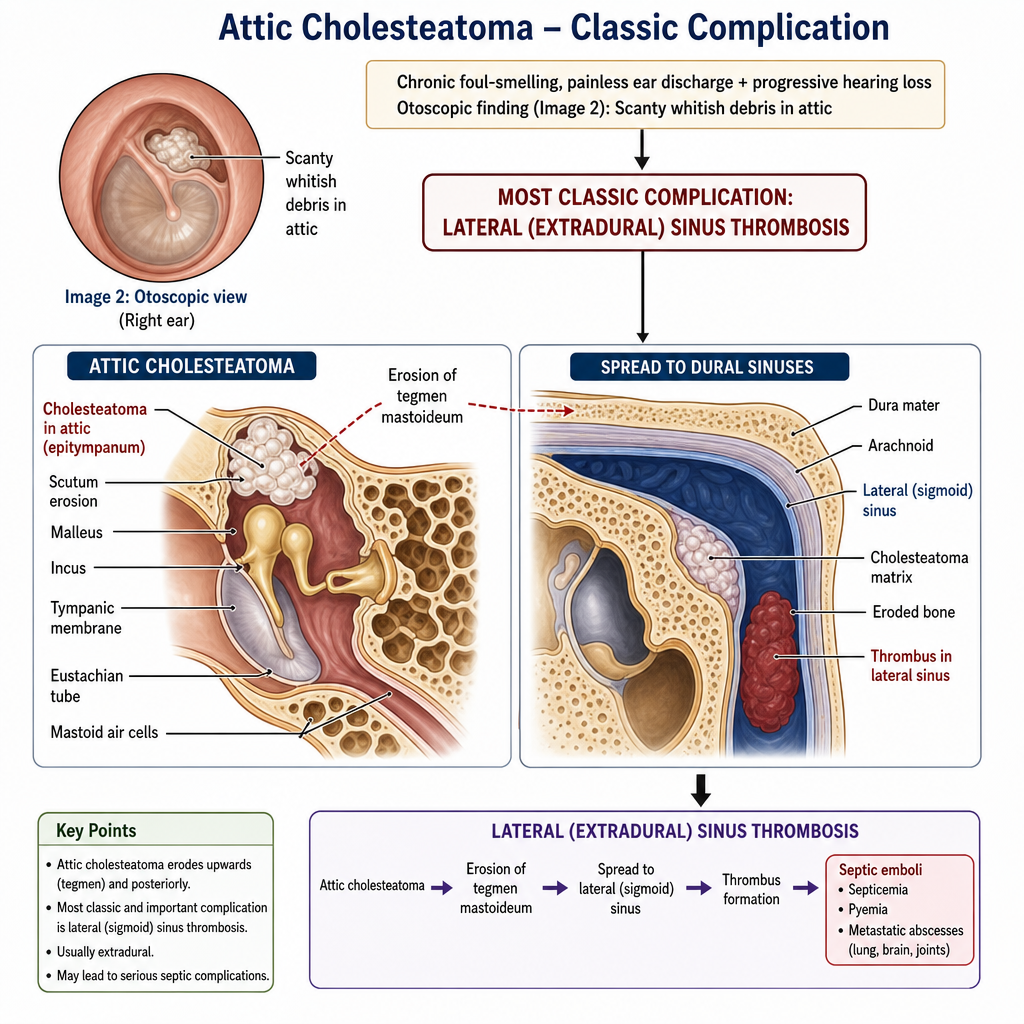
A 45-year-old man presents with a 6-month history of foul-smelling unilateral ear discharge and progressive right-sided hearing loss. He denies pain or vertigo. On examination, the ear canal contains scanty whitish debris. His otoscopic image is shown (Image 2). Which of the following complications is most classically associated with this attic cholesteatoma?
Practice by Chapter
Otitis Externa
Practice Questions
Acute Otitis Media
Practice Questions
Chronic Otitis Media
Practice Questions
Complications of Otitis Media
Practice Questions
Otosclerosis
Practice Questions
Presbycusis
Practice Questions
Sudden Sensorineural Hearing Loss
Practice Questions
Noise-Induced Hearing Loss
Practice Questions
Ménière's Disease
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Tumors of the Ear and Temporal Bone
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app