
Audiology and Speech Disorders — MCQs

On this page
What is the standard frequency used in tympanometry?
In right-sided middle ear pathology, what will be the finding in Weber's test?
In which of the following conditions is the threshold for bone conduction normal and the threshold for air conduction increased?
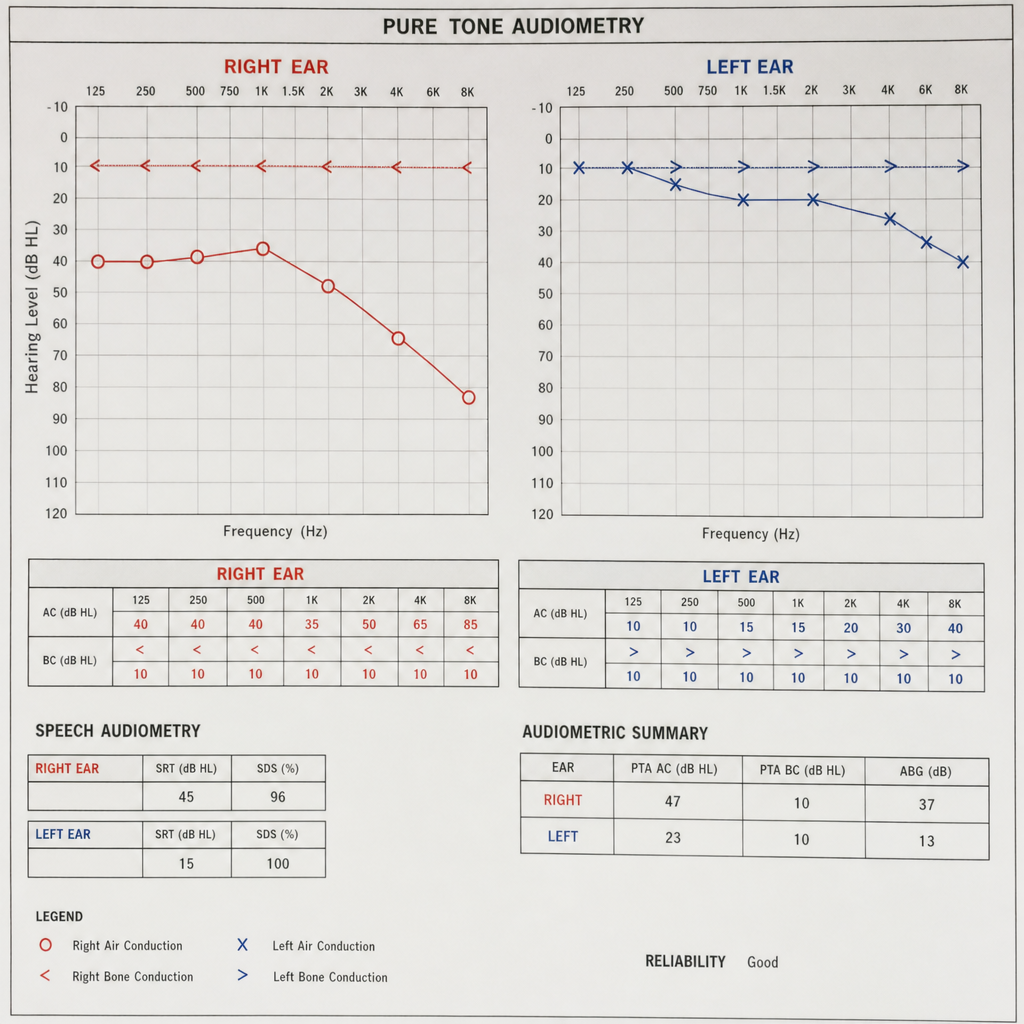
An audiometry report is provided. Interpret the audiogram to determine which ear has the more severe conductive hearing loss.
What is the investigation of choice for audiometric evaluation of an infant?
Rinne test is negative in which of the following conditions?
What is the threshold for moderate hearing loss?
Stapedial reflex is absent in:
A B-type tympanogram is typically seen in which of the following conditions?
Otoacoustic emissions arise from which structure?
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app