
Audiology and Speech Disorders — MCQs

On this page
Type Ad curve in tympanometry is seen in which of the following conditions?
Deafness is seen with which of the following conditions?
Type Ad curve is seen in?
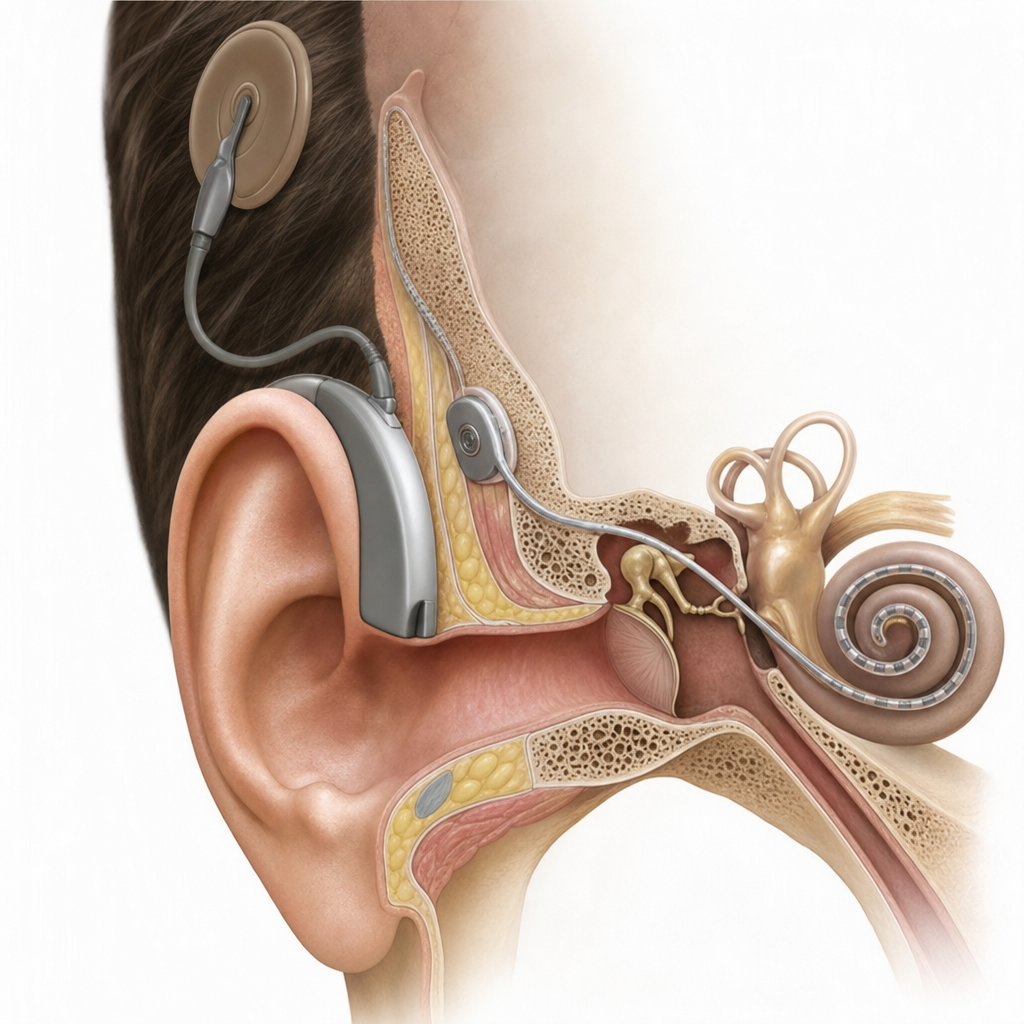
Which device is shown below?
Carhart's notch in an audiogram represents the deepest frequency loss at which of the following frequencies?
Auditory screening is required in children under which of the following conditions?
Subjective interference is present in which of the following audiological tests?
Cochlear implant is indicated at the minimum age of?
A patient presents with a hearing defect. His tuning fork test results were: Weber test - sound from a vibrating tuning fork was louder than normal; Schwabach test - bone conduction was better than normal; and Rinne test - air conduction did not outlast bone conduction. What is the most likely diagnosis?
A person hears two different tones in the left and right ear when presented with a single tone. What is this condition called?
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app