
Audiology and Speech Disorders — MCQs

On this page
Loudness recruitment phenomenon is associated with which type of hearing loss?
What are the indications for a brain stem implant in a two-year-old child?
A cochlear implant can be used in all of the following conditions causing bilateral severe to profound hearing loss, except:
In the Bing test, alternately compressing and relaxing the tragus causes the sound to increase and decrease. This finding indicates:
Acoustic reflex is lost in case of which of the following conditions?
Otoacoustic emissions arise from which structures?
Rinne's test is negative in which of the following conditions?
Which of the following is not a cause of conductive hearing loss?
Which of the following is NOT true about otoacoustic emissions?
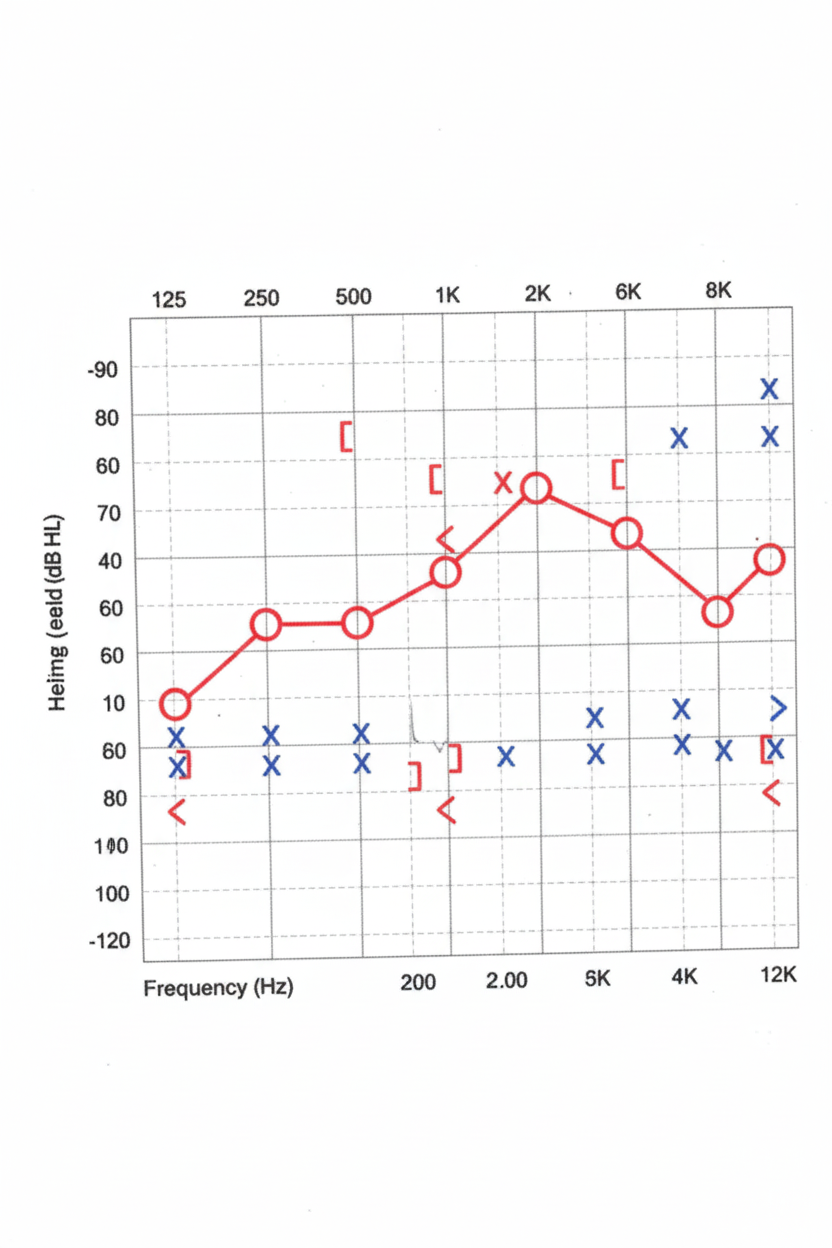
A 30-year-old female presents with hearing loss. An audiogram is obtained. What is her most likely diagnosis?
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app