
Audiology and Speech Disorders — MCQs

On this page
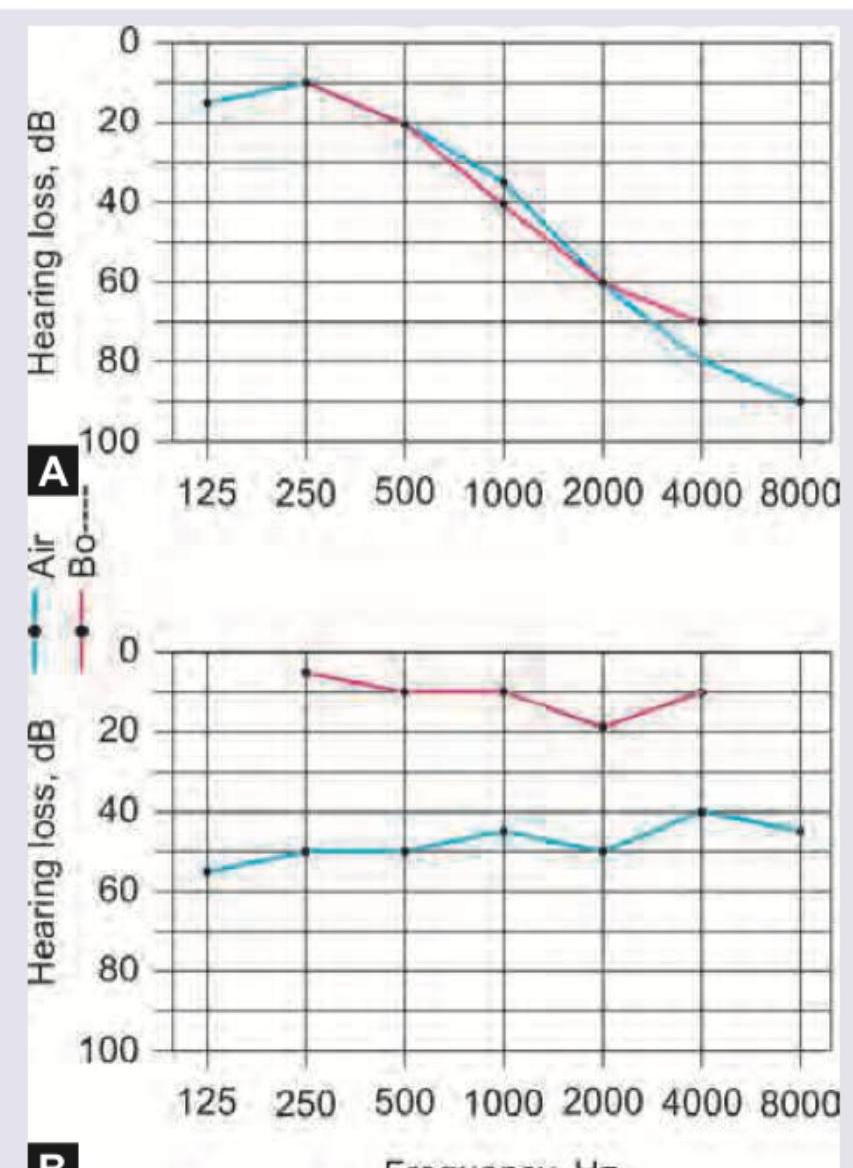
Which is correct about the pure tone audiometry tracing given below?
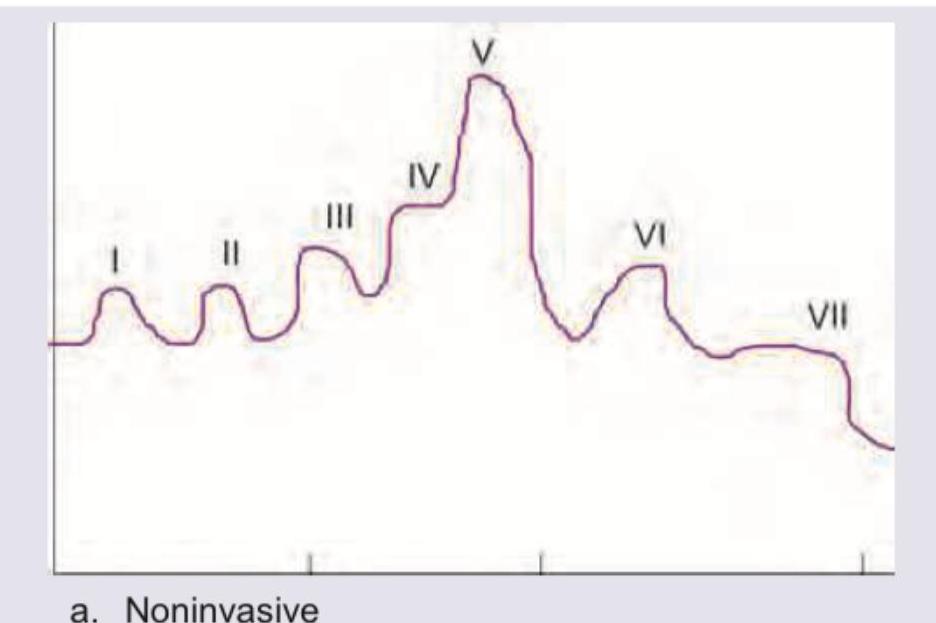
All are true about the click-evoked ABR recording shown in the image except:
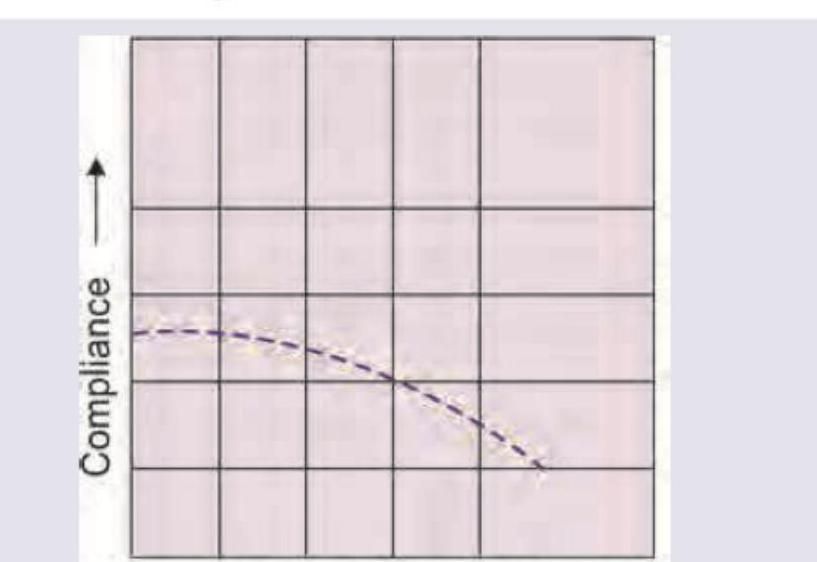
The tympanogram shown below is seen in which of the following conditions?
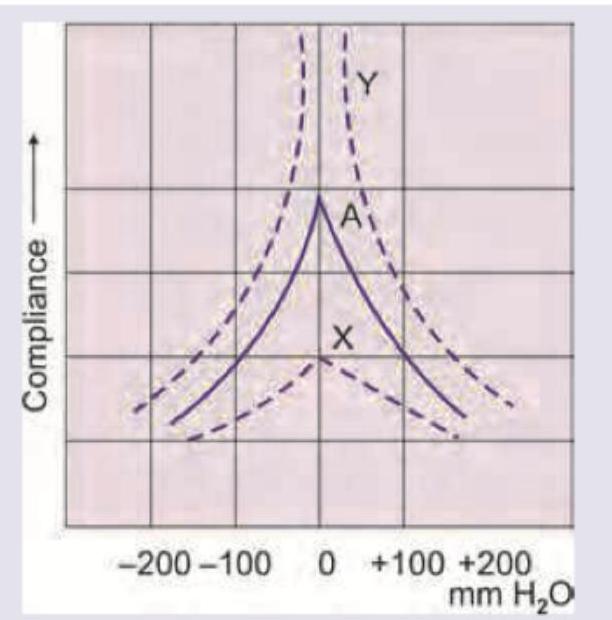
The tympanogram shown below is seen in which of the following conditions?
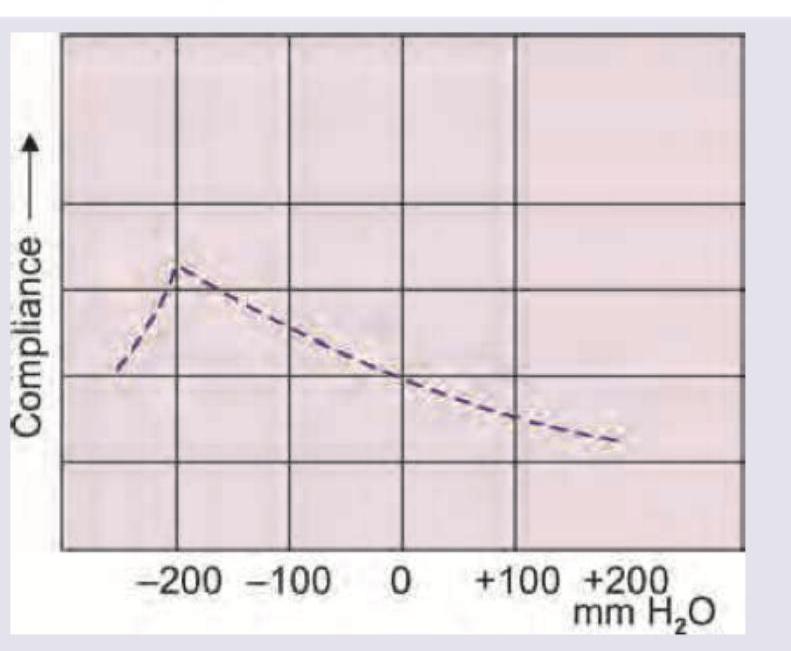
The tympanogram shown below is seen in which of the following conditions?
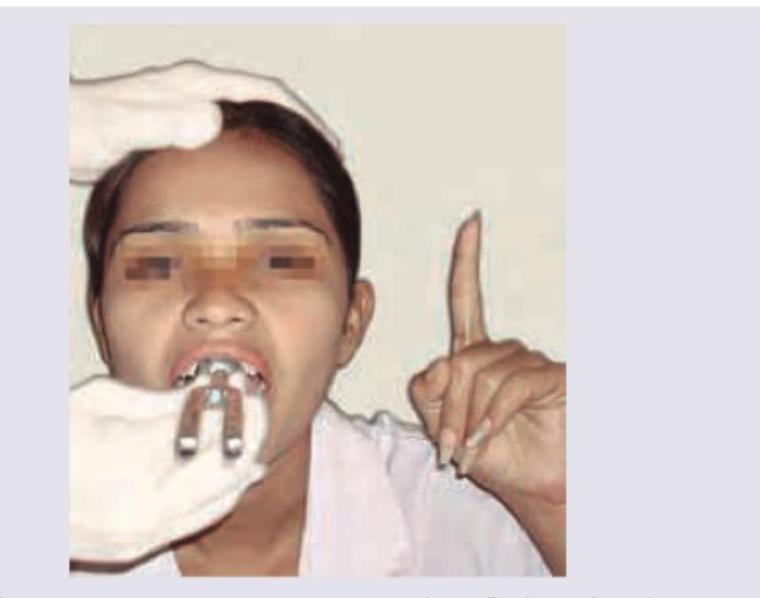
Which test is being performed in the patient?
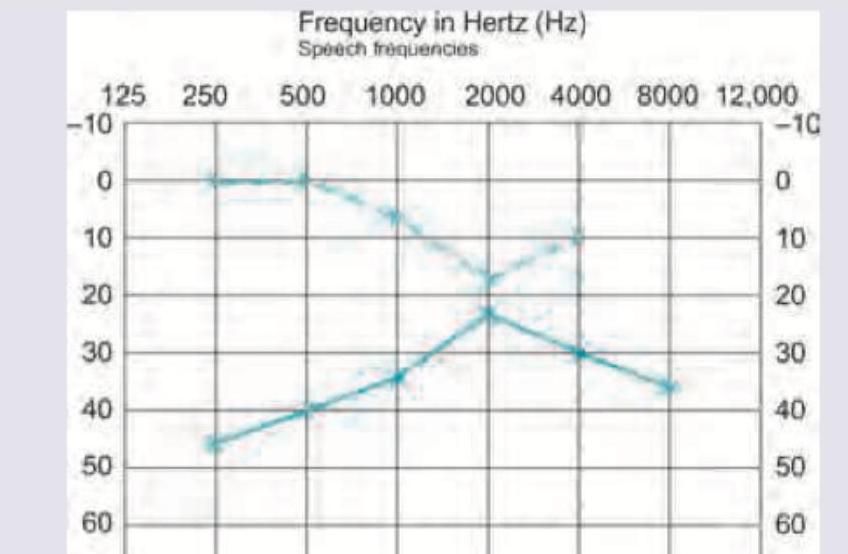
Which of the following is the diagnosis of the audiogram shown below?
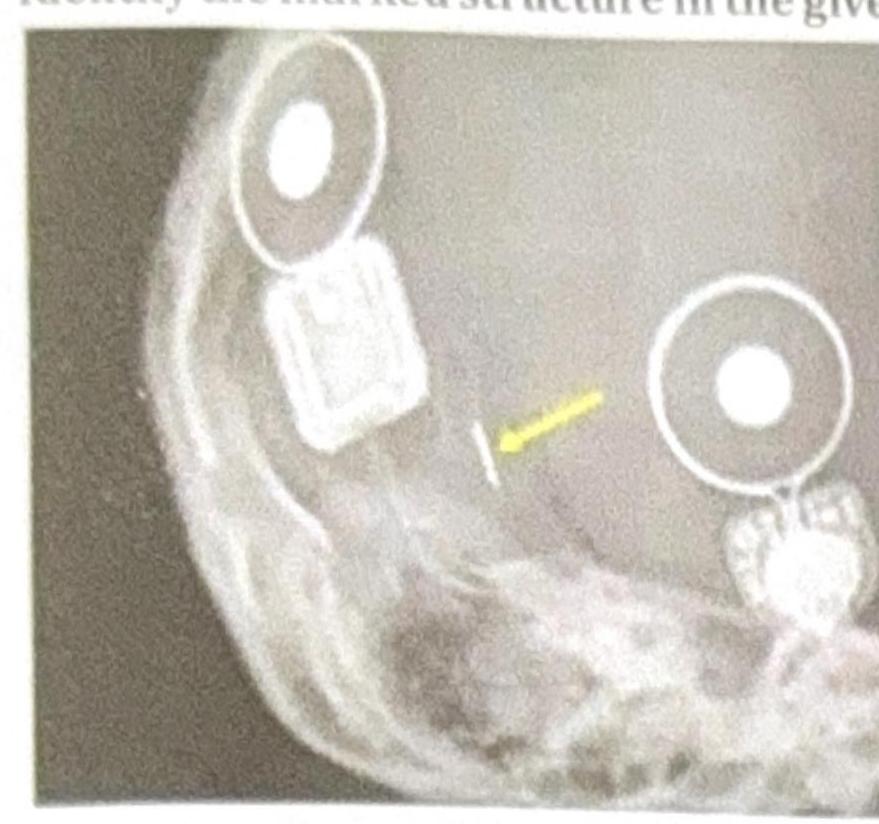
Identify the marked structure in the given image.
A 14-year-old female patient presents to the ENT OPD and complains that she can hear sounds clearly but has difficulty processing and understanding what is being said. Her Pure tone audiometry and ABR are normal. What is the likely diagnosis in this patient?
Dip at 4000 Hz in pure tone audiometry indicates:
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app