
Audiology and Speech Disorders — MCQs

On this page
Which of the following is true about the image provided?

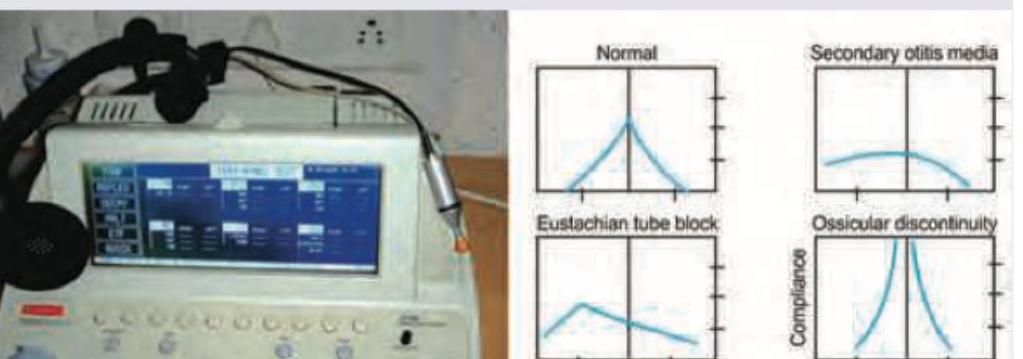
Which of the following best describes the principle of the test being performed?

All of the following are early complications of cochlear implant surgery shown except:
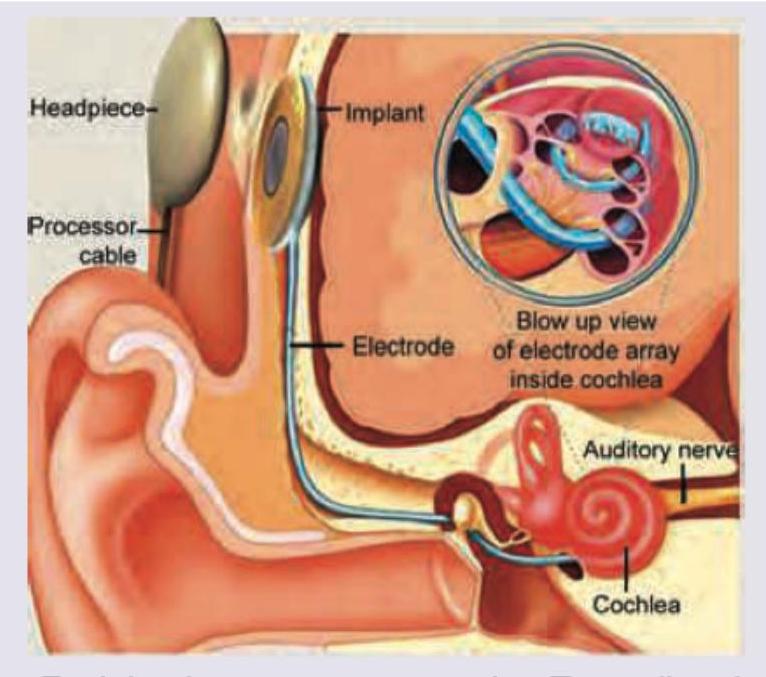
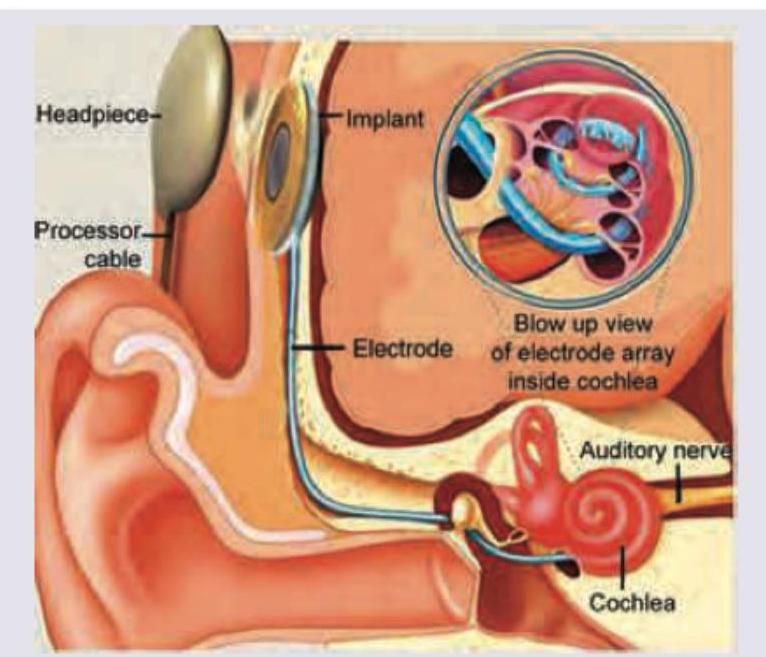
Which of the following hearing aid or implant is shown below?
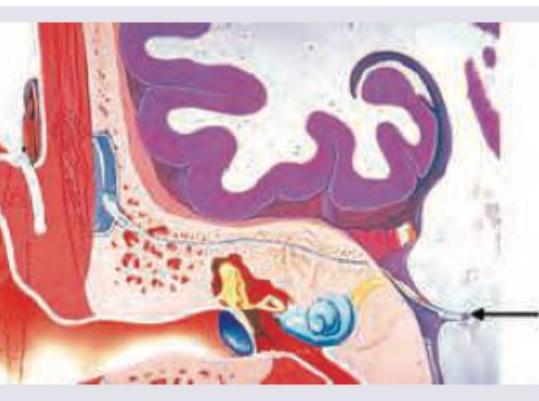
The electrode of the hearing implant shown below is placed in:
All of the following are true about the hearing aid shown in the figure except:
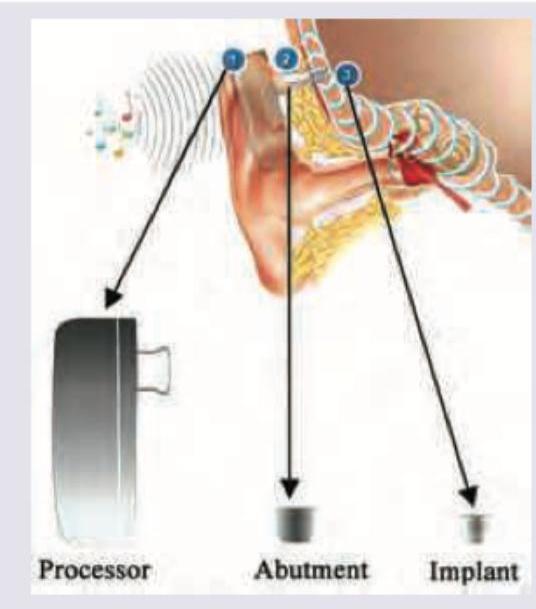
Which type of hearing aid is shown below?
The following test is useful for diagnosis of all except:
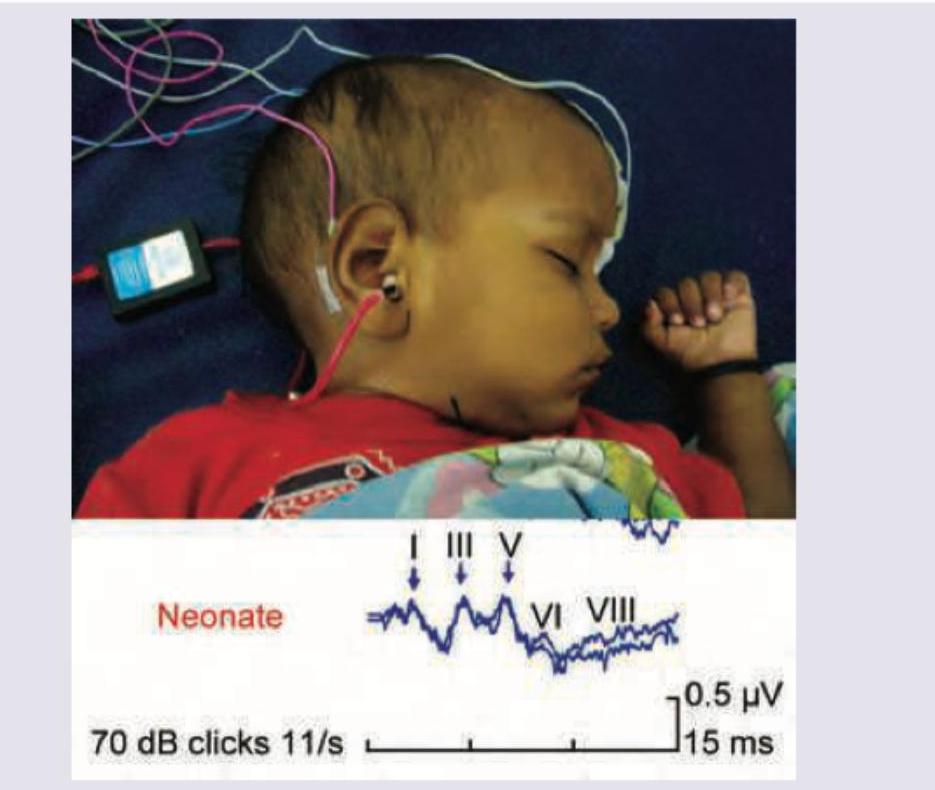
A 1-year-old child has spastic cerebral palsy. Which of the following tests is being performed on the child?
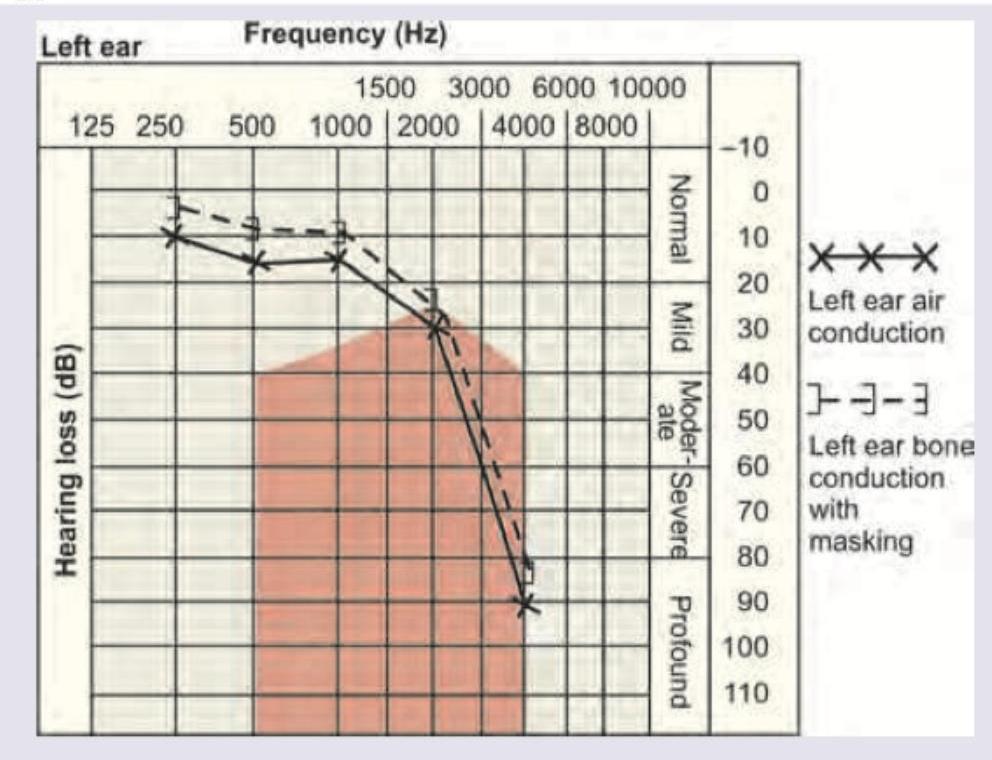
The audiogram shown below denotes:
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app