
Audiology and Speech Disorders — MCQs

On this page
Which is the best screening test to evaluate hearing in a neonate?
Which test is used to detect damage to the cochlea?
All of the following are subjective tests for audiometry except:
A tympanometry graph is shown below. An arrow indicates a shallow peak at pressure = 0 daPa. What is the most likely diagnosis based on the tympanometry result shown?
A patient presents to the OPD with hearing loss. On examination: - Rinne test - Positive in the left ear and negative in the right ear - Weber's test - lateralization towards the left - Bone conduction test - Reduced in the right ear and similar in the left ear. Interpret the findings.
What is the most commonly used test for newborn hearing screening?
Choose the most appropriate candidates for cochlear implants: 1. Ototoxicity 2. Congenital hearing loss 3. Ossicular fixation 4. Otosclerosis
A 30-year-old male presents to the clinic with a history of recurrent ear infections and a recent "popping" sensation in his left ear. Otoscopic examination of the left ear reveals a central perforation of the tympanic membrane. The pure tone audiometry (PTA) results show the following: Right Ear: Air conduction and bone conduction thresholds are within normal limits. Left Ear: A significant air-bone gap is present, with bone conduction thresholds within the normal range. Based on these findings, what is the most likely diagnosis regarding the type of hearing loss?
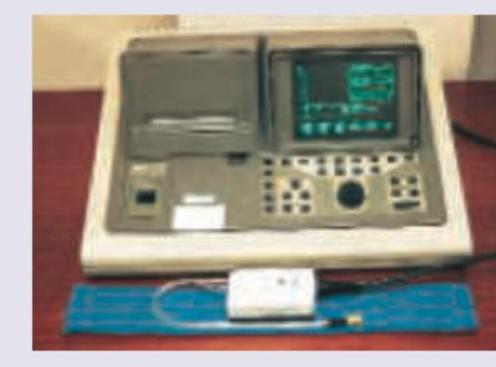
Identify the device shown in the image below:

The instrument shown below is used in ENT for all except: (Recent NEET Pattern 2016-17)
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app