
Bone-Anchored Hearing Devices — MCQs

A 65-year-old patient presents with gradual progressive hearing loss over several years. Rinne test shows bone conduction > air conduction bilaterally. Weber test lateralizes to the worse ear. Tympanic membranes are intact and normal. Which is the most likely diagnosis?
Most common bone affected by otosclerosis?
A 45-year-old gentleman reports decreased hearing in the right ear for the last two years. On testing with a 512 Hz tuning fork, the Rinne's test without masking is negative on the right ear and positive on the left ear. With the Weber's test, the tone is perceived as louder in the left ear. Patient most likely has -
Which anatomical structure serves as the passageway connecting the middle ear cavity to the mastoid air cells, allowing the spread of infection?
Which of the following statements about Bone Anchored Hearing Aids (BAHA) is true?
What type of prosthesis is commonly used during stapes surgery for otosclerosis?
Which of the following is not a function of the instrument given below?

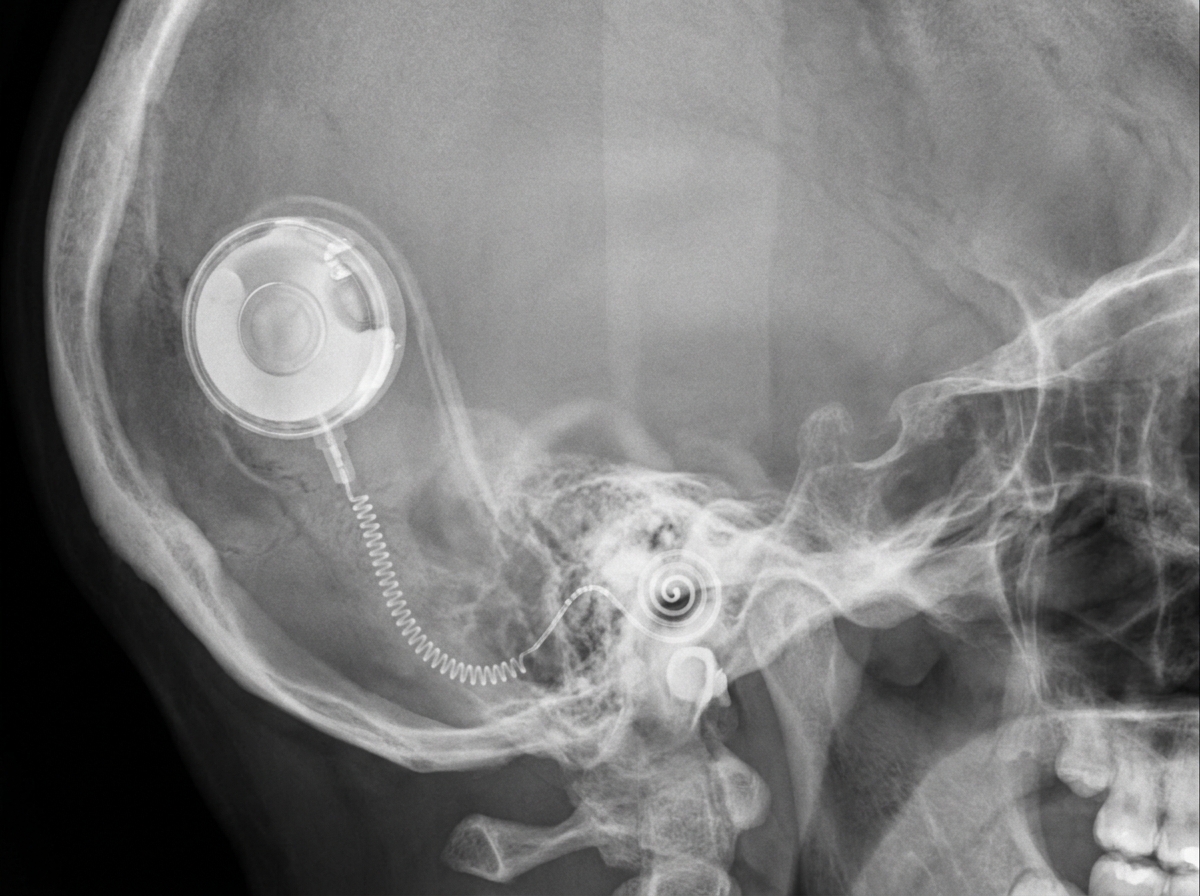
Which device is depicted below?
What should be the minimum hearing loss for Weber's test to lateralize?
A pure tone audiogram showing a bone conduction dip (Carhart notch) at 2000 Hz is characteristic of-
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app