
Audiology and Speech Disorders — MCQs

On this page
A 10-year-old boy presented with sensorineural deafness not benefited with a hearing aid. What is the next treatment?
In right middle ear pathology, where will the Weber's test lateralize?
Brainstem Evoked Response Audiometry (BERA) can be most accurately performed from which gestational age?
What is the screening investigation for suspected hearing loss in high-risk neonates admitted to the ICU?
All of the following are tuning fork tests to differentiate hearing loss, EXCEPT:
What is the ideal hearing aid for a patient with anotia?
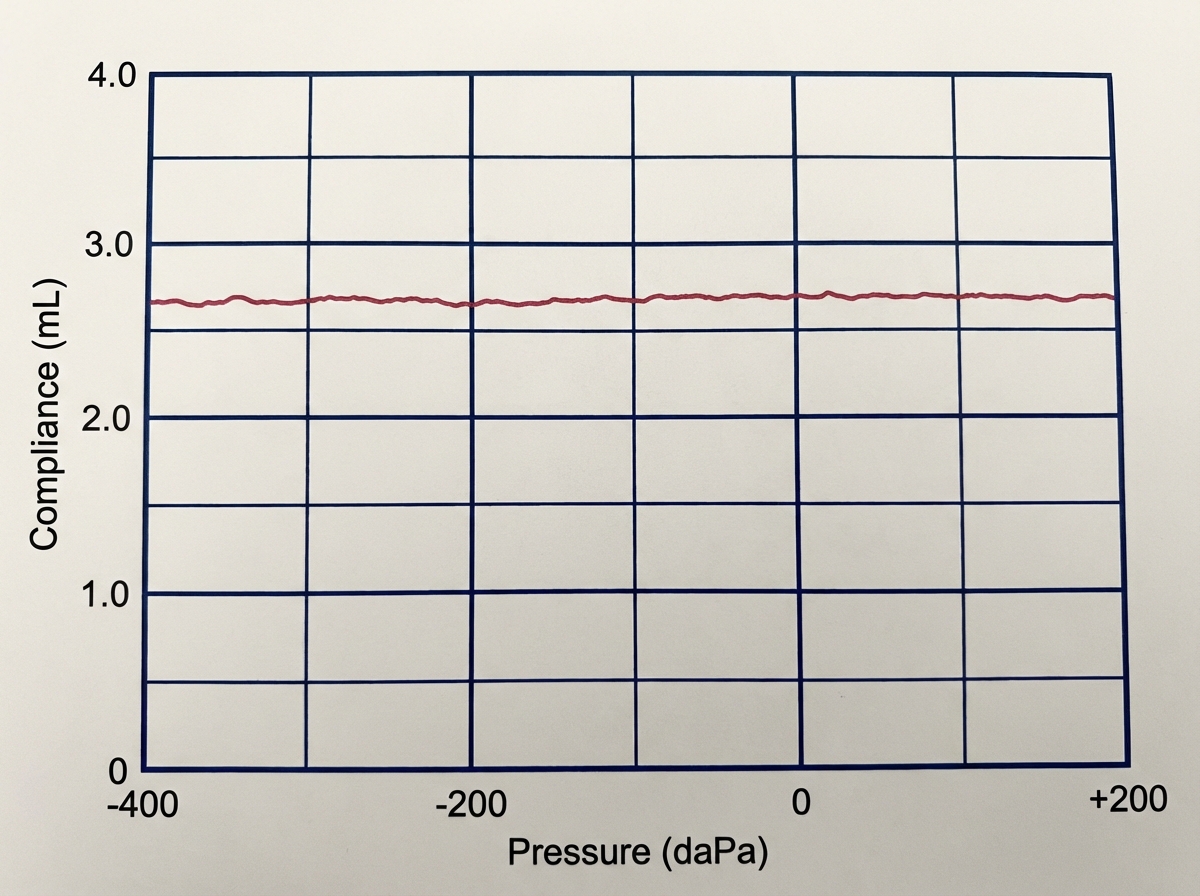
This tympanogram is seen in which of the following conditions?
In noise-induced hearing loss, the audiogram typically shows a dip (Boiler's notch) at which frequency?
Wave V in Brainstem Evoked Response Audiometry (BERA) typically corresponds to which neural pathway or structure?
All are true about cochlear implant except?
Practice by Chapter
Hearing Assessment Techniques
Practice Questions
Tympanometry and Acoustic Reflexes
Practice Questions
Otoacoustic Emissions
Practice Questions
Auditory Brainstem Response
Practice Questions
Hearing Aids
Practice Questions
Cochlear Implants
Practice Questions
Bone-Anchored Hearing Devices
Practice Questions
Speech and Language Development
Practice Questions
Articulation Disorders
Practice Questions
Stuttering
Practice Questions
Dysphonia
Practice Questions
Rehabilitation of Hearing-Impaired Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app