
Viral Infections in Immunocompromised Hosts — MCQs

AIDS, secondary infection will be all except
A 65-year-old patient presents with symptoms of bone pain, anemia, hypercalcemia, and renal impairment. A bone marrow biopsy confirms the diagnosis of multiple myeloma. The patient is started on a treatment regimen. Which of the following treatments is most likely associated with the reactivation of herpes zoster?
What could be the most appropriate provisional diagnosis for multiple nodular exophytic reddish lesions of oral mucosa in an AIDS patient?
Which of the following statements about molluscum contagiosum is FALSE?
A patient on steroids develops sudden onset painful vesicles in T4 dermatome. Best initial treatment is:
A 19-year-old woman presents with painful genital ulcers and vesicles for 4 days, accompanied by fever, malaise, and tender inguinal lymphadenopathy. What is the most appropriate initial management?
In which condition are Bull's eye lesions typically found?
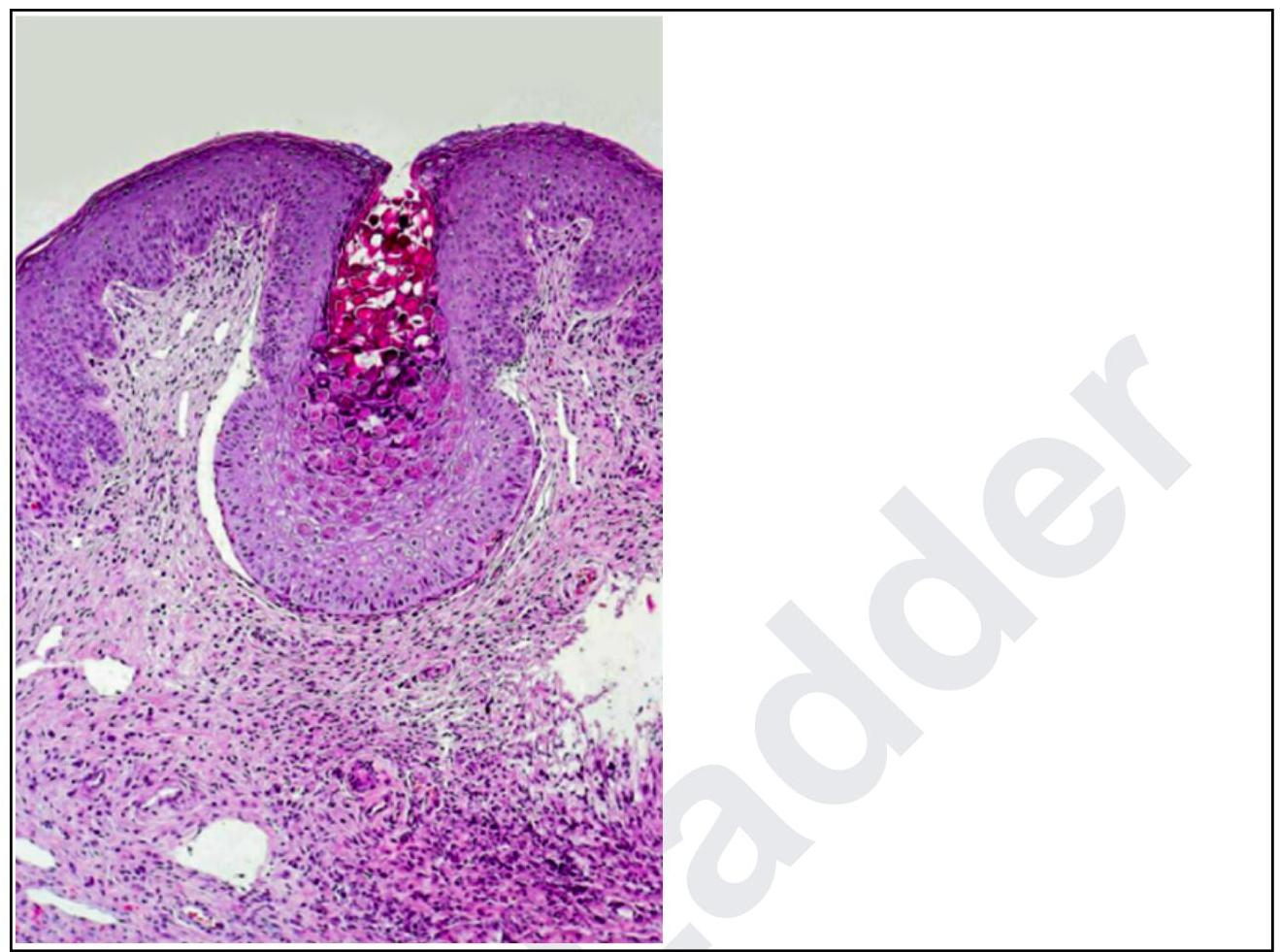
A woman presents with lesions on the inner thighs and peri-anal region. They are nodular, 4-6 mm in size and appear pale. The histopathological image shows multiple intracytoplasmic inclusion bodies consistent with Henderson-Patterson bodies. The diagnosis is:
In HIV patients, Kaposi's sarcoma is most likely caused by which of the following?
Neonatal conjunctivitis is caused by all of the following except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app