
Viral Skin Infections — MCQs

On this page
A patient developed fever and perioral vesicles. What is the diagnosis?

A 28-year-old lady has asymptomatic dome shaped small lesions on the forehead for the last 2 months as shown in the image. She has a 2-year-old daughter with similar lesions. What is the causative agent? (AIIMS May 2016)
All are true about the lesion shown in the image except:

All are true about the lesion shown in the image except:

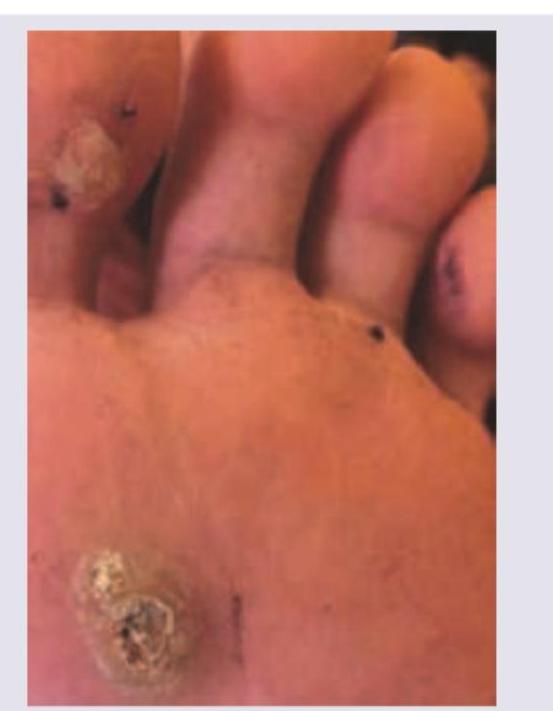
A 25-year-old athlete presents with the following painless lesions in the sole of the foot. The aetiology is:
Which is not correct about the lesion shown below?

A 28-year-old lady has asymptomatic dome-shaped small lesions on the forehead for the past 2 months. She lives with her 2-year-old daughter who also is having similar lesions. What is the causative agent of these lesions?
Which of the following is INCORRECT regarding genital warts (condyloma acuminata)? 1. It is usually single. 2. It is related to HPV Types 6 and 11. 3. It can be transmitted sexually. 4. It can involve vagina and anus.
Which of the following statements about molluscum contagiosum is FALSE?
A 19-year-old woman presents with painful genital ulcers and vesicles for 4 days, accompanied by fever, malaise, and tender inguinal lymphadenopathy. What is the most appropriate initial management?
Practice by Chapter
Herpes Simplex Virus Infections
Practice Questions
Varicella-Zoster Virus Infections
Practice Questions
Human Papillomavirus Infections
Practice Questions
Molluscum Contagiosum
Practice Questions
Viral Exanthems
Practice Questions
Hand, Foot, and Mouth Disease
Practice Questions
Orf and Milker's Nodule
Practice Questions
Cytomegalovirus Cutaneous Manifestations
Practice Questions
Epstein-Barr Virus Manifestations
Practice Questions
Poxvirus Infections
Practice Questions
HIV-Related Dermatoses
Practice Questions
Viral Infections in Immunocompromised Hosts
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app