
Viral Skin Infections — MCQs

On this page
Identify the infectious cause of erythema multiforme in the image.

Which of the following conditions is caused by Human Papillomavirus (HPV)?
What is the most probable diagnosis of a child who presents with white umbilicated lesions on the face?
Which of the following statements about herpes zoster complications is incorrect?
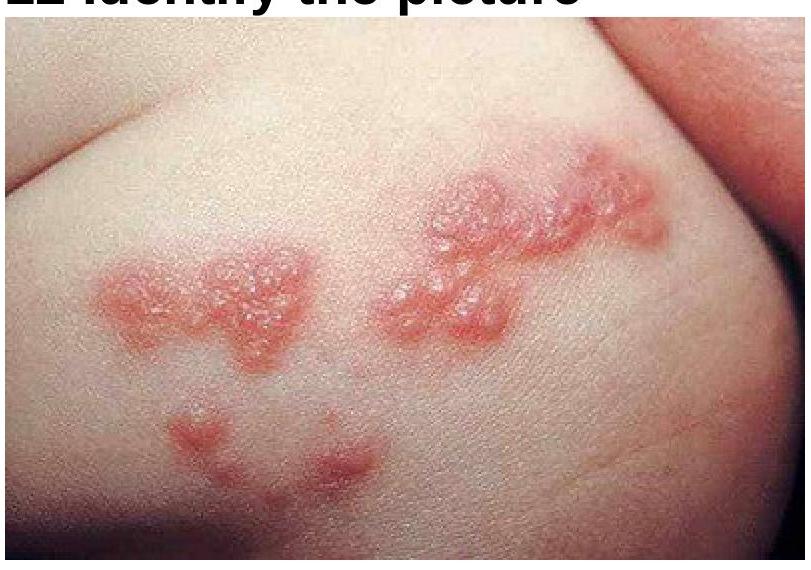
A patient presents with painful vesicular eruptions on one side of the body. What is the most likely diagnosis based on the clinical image?
A child with a family history of allergies presents with pruritus on the face and convexities, followed by the development of numerous umbilicated vesicles that become pustular, hemorrhagic, and crusted. After two days, the child develops a high fever and lymphadenopathy. What is the most likely diagnosis?
Which area is typically not involved in a chickenpox rash?
A man with pain during defecation, no gastrointestinal symptoms, and ulcers extending into the anal canal. Diagnosis?
What does a Tzanck smear in varicella-zoster virus infection typically show?
What is the most common trigger associated with erythema multiforme?
Practice by Chapter
Herpes Simplex Virus Infections
Practice Questions
Varicella-Zoster Virus Infections
Practice Questions
Human Papillomavirus Infections
Practice Questions
Molluscum Contagiosum
Practice Questions
Viral Exanthems
Practice Questions
Hand, Foot, and Mouth Disease
Practice Questions
Orf and Milker's Nodule
Practice Questions
Cytomegalovirus Cutaneous Manifestations
Practice Questions
Epstein-Barr Virus Manifestations
Practice Questions
Poxvirus Infections
Practice Questions
HIV-Related Dermatoses
Practice Questions
Viral Infections in Immunocompromised Hosts
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app