
Orf and Milker's Nodule — MCQs

A child presented with bluish-white spots in the mouth followed by a rash. What is the genome of the most likely causative agent?
An infant presented with the following lesions on his face and limbs. Which of the following is the most likely causative organism?

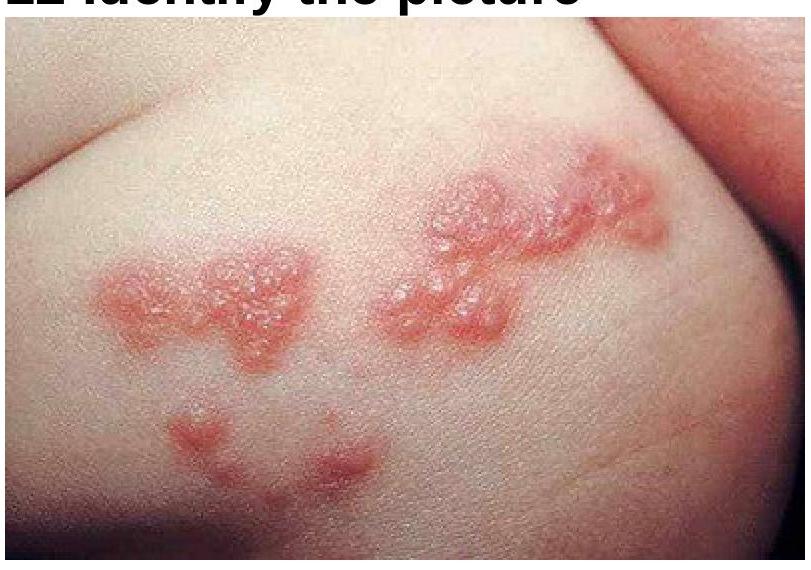
A patient presents with painful vesicular eruptions on one side of the body. What is the most likely diagnosis based on the clinical image?
Fever of unknown origin in a farmer who raises goats would most likely be caused by which of the following organisms?
Which of the following clinical manifestations is LEAST likely in secondary syphilis?
Which of the following does not have a viral etiology?
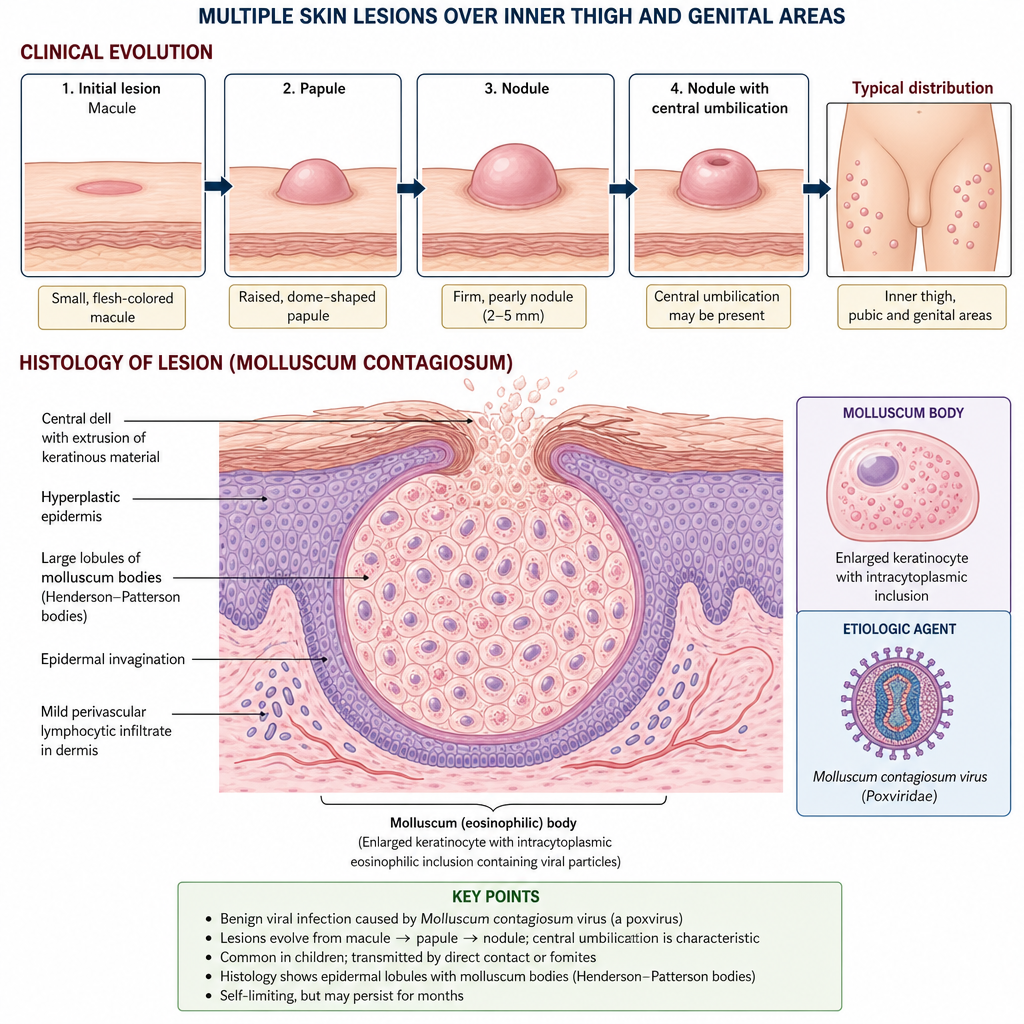
A child presents with multiple skin lesions over the inner thigh and genital areas. It initially started as macule and later developed to become nodules. Some nodules have central umbilication. The histology of the lesion is shown below
All are true about erythema multiforme except which of the following?
Identify the lesion: (Recent NEET Pattern 2016-17)

An individual develops a high-grade fever lasting for 3 days, after which a vesicular rash appears. The rash is predominantly centripetal, involving the trunk more than the extremities, as shown in the image. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app