
Tropical Dermatology — MCQs

On this page
A 7-year-old child presents with a hypopigmented, anesthetic patch on the face. What is the most probable diagnosis?
All the features of peripheral neuritis in a patient with Hansen's disease EXCEPT?
What is the treatment for lepra reaction with acute neuritis?
An 8-year-old boy presents with a 6-month history of an ill-defined, hypopigmented, slightly atrophic macule on the face. What is the most likely diagnosis?
What is the drug of choice for Erythema Nodosum Leprosum?
Which of the following oral structures are not affected in Leprosy?
The following presentation is called:

A 65-year-old beggar comes to your OPD with following presentation in upper part of foot. Gram stain of discharge was performed and demonstrates eumycetoma. All are true about the condition shown except:
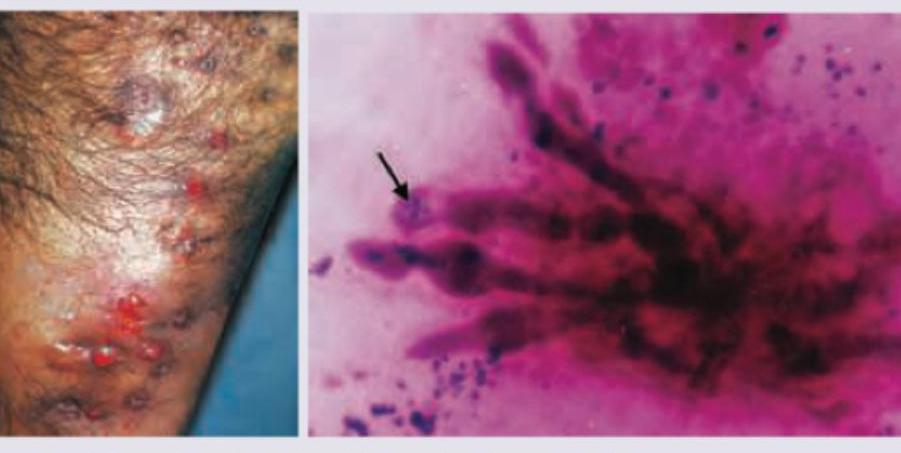
The image shows:

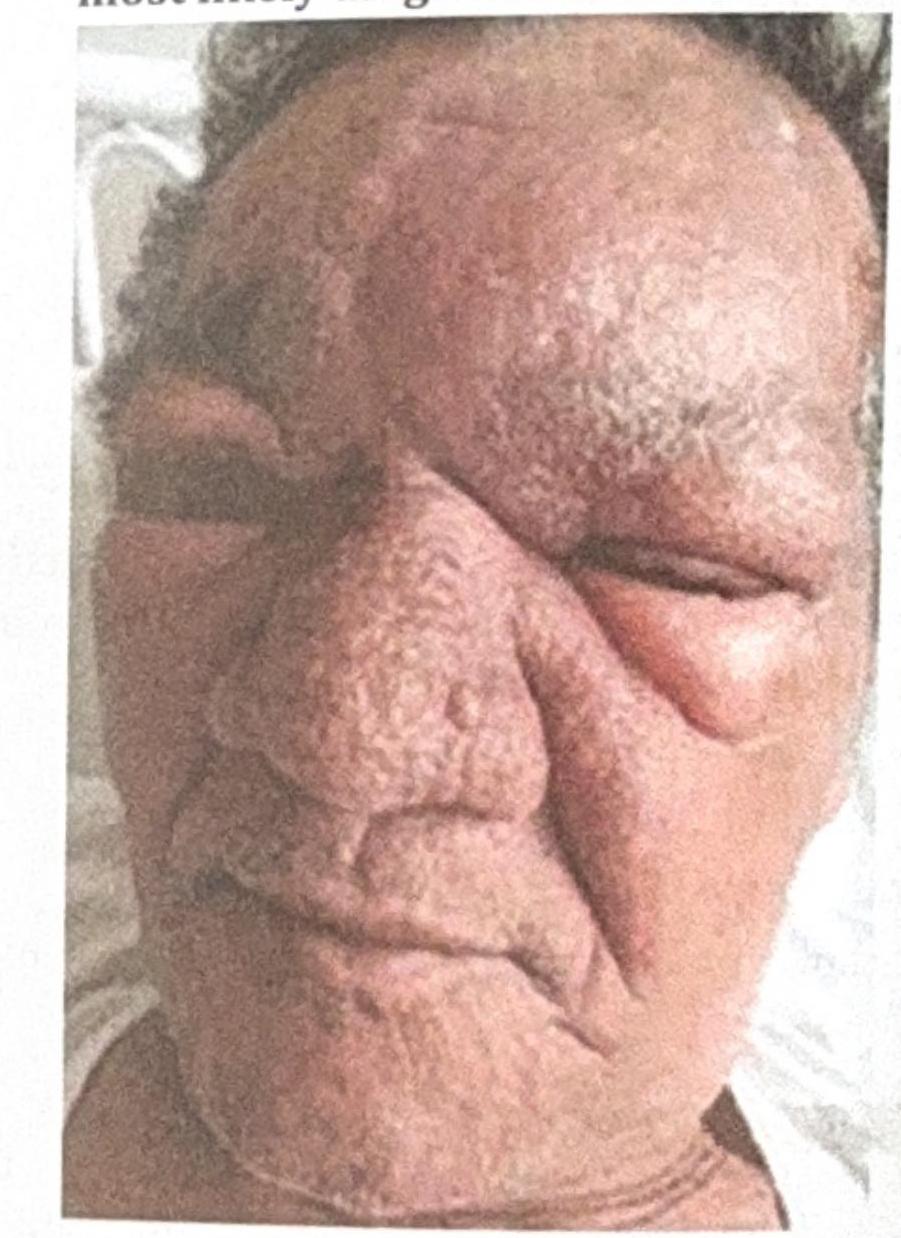
A 53 year-old male presented with erythematous, edematous plaques on his face over pre-existing hypoesthetic patches. He has been experiencing pain for the last 10 days and has been on multibacillary multidrug therapy (MBMDT) for leprosy for the past two months. What is the most likely diagnosis based on the image?
Practice by Chapter
Cutaneous Leishmaniasis
Practice Questions
Leprosy
Practice Questions
Tropical Ulcers
Practice Questions
Onchocerciasis
Practice Questions
Filariasis
Practice Questions
Tropical Mycoses
Practice Questions
Cutaneous Larva Migrans
Practice Questions
Tungiasis
Practice Questions
Myiasis
Practice Questions
Cutaneous Manifestations of Malaria
Practice Questions
Dengue and Other Viral Hemorrhagic Fevers
Practice Questions
Global Health Perspectives in Dermatology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app