
Skin Tumors — MCQs

On this page
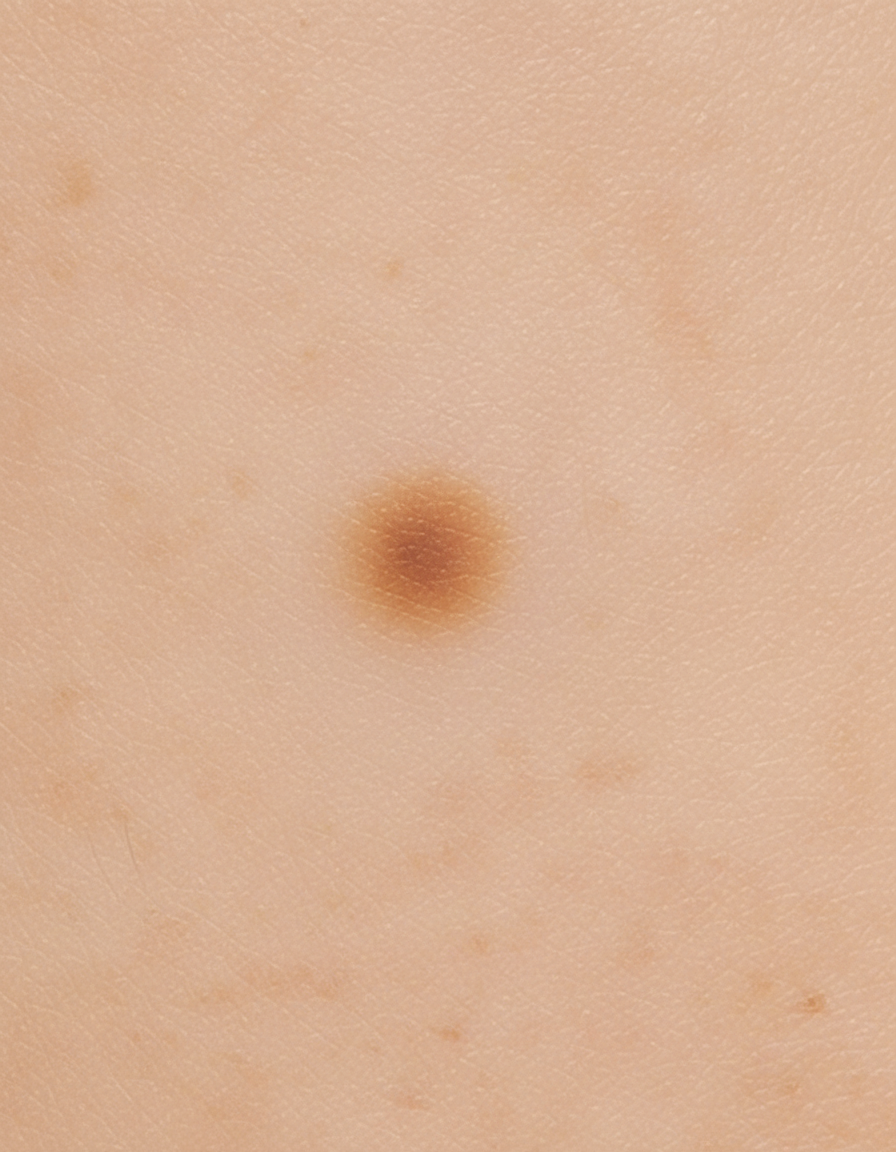
Identify the type of skin lesion shown in the image.
Which of the following statements about keloids is MOST true?
Which of the following statements about Bowen's disease is correct?
In which part of the body are lesions of Kaposi sarcoma most commonly seen?
All of the following are premalignant conditions except which of the following?
What is the most likely diagnosis for a 15 mm hyperpigmented lesion on the shoulder that is enlarging and has hair growing from it?
A 15cm hyperpigmented macule on an adolescent male undergoes changes such as coarseness, growth of hair & acne. Diagnosis is?
Muir–Torre syndrome shows
What is the most common cancer associated with a burn scar?
Which of the following is a common differential diagnosis of verrucous carcinoma?
Practice by Chapter
Benign Epithelial Tumors
Practice Questions
Premalignant Epidermal Tumors
Practice Questions
Basal Cell Carcinoma
Practice Questions
Squamous Cell Carcinoma
Practice Questions
Melanocytic Nevi
Practice Questions
Melanoma
Practice Questions
Merkel Cell Carcinoma
Practice Questions
Vascular Tumors and Malformations
Practice Questions
Cutaneous Lymphomas
Practice Questions
Soft Tissue Tumors
Practice Questions
Metastatic Skin Tumors
Practice Questions
Skin Cancer Prevention and Screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app