
Skin Tumors — MCQs

On this page
A 70-year-old man presents with non-healing, pearly nodules on his face. What is the most likely diagnosis?
A 55-year-old male presents with an ulcerative lesion on his leg that does not heal despite treatment. Which condition should be considered?
What is the most common type of cutaneous mastocytosis?
Acral lentiginous type of malignant melanoma occurs in -
Visual examination is used as a screening test for skin cancer in adults. Among the following skin lesions/cancers, which is considered most important to detect through this visual screening method?
What is the color of tuberous sclerosis lesions when examined under a Wood's lamp?
A male patient presented with a 0.3 cm nodule on the left nasolabial fold. A pathological examination revealed a basaloid appearance with peripheral palisading. What is the most likely diagnosis?

Elderly man with a long-standing mole on his face that is increasing in size and showing an irregular border. Diagnosis:
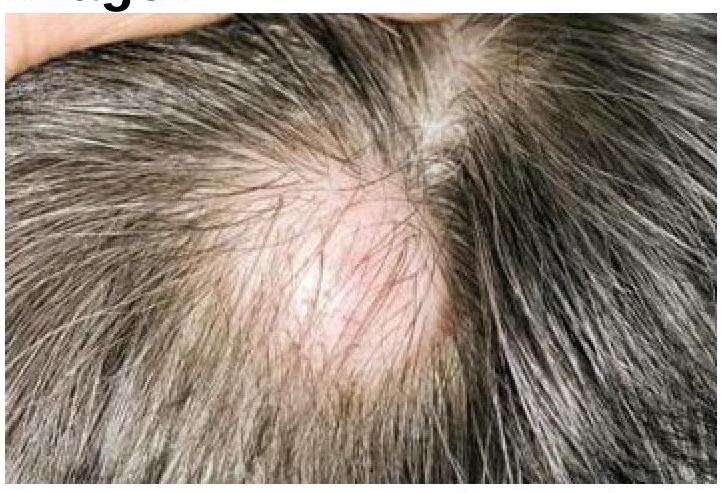
Identify the condition shown in the image.
Which of the following is the MOST significant risk factor for cutaneous lymphoma?
Practice by Chapter
Benign Epithelial Tumors
Practice Questions
Premalignant Epidermal Tumors
Practice Questions
Basal Cell Carcinoma
Practice Questions
Squamous Cell Carcinoma
Practice Questions
Melanocytic Nevi
Practice Questions
Melanoma
Practice Questions
Merkel Cell Carcinoma
Practice Questions
Vascular Tumors and Malformations
Practice Questions
Cutaneous Lymphomas
Practice Questions
Soft Tissue Tumors
Practice Questions
Metastatic Skin Tumors
Practice Questions
Skin Cancer Prevention and Screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app