
Skin Tumors — MCQs

On this page
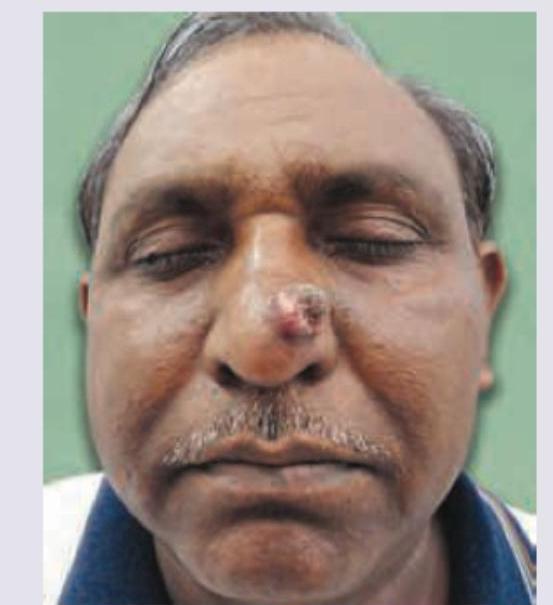
A 50-year-old patient presents with lesion over the nose with rapid growth for last 6 weeks. He has no past history of any skin disease. The image shows presence of?
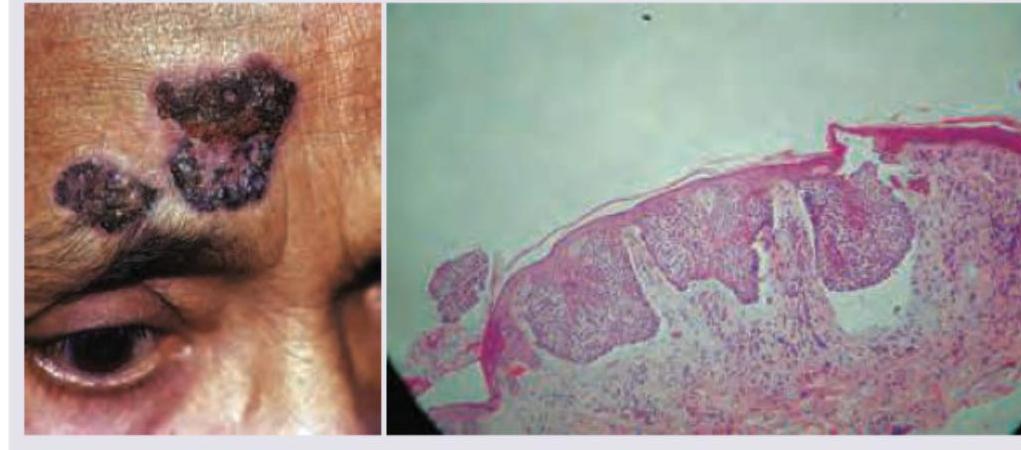
A 70-year-old man presents with an ulcerative lesion over the forehead. A biopsy was performed. All are true about the condition shown except?
A 25 -year-old patient presents with multiple sebaceous adenomas over the neck and chest. His father too had a similar skin disease and died due to colorectal carcinoma. What is the diagnosis?
Identify the condition which is present since birth: (AIIMS May 2017)
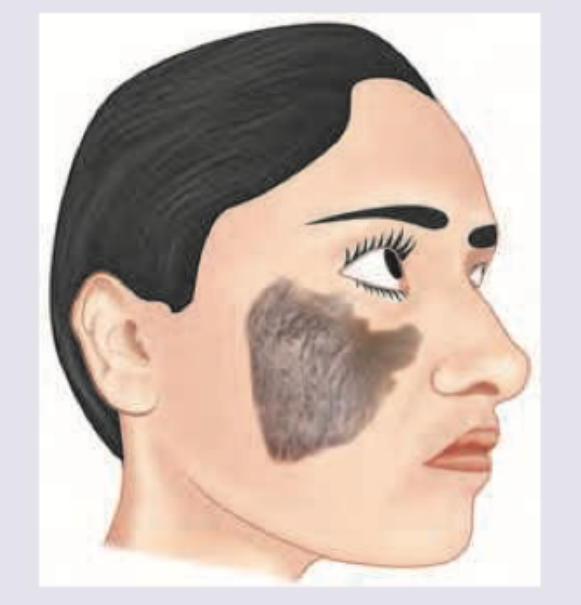
What is the best management of the case shown?
The following lesion was noticed in a patient with history of involuntary weight loss. The lesions appeared suddenly and increased rapidly in number. What is the diagnosis?

A 38-year-old man presents with the manifestation shown in the image. He has a number of family members suffering from the same condition, though the severity is different in different members. Which of the following statements is false regarding this condition?

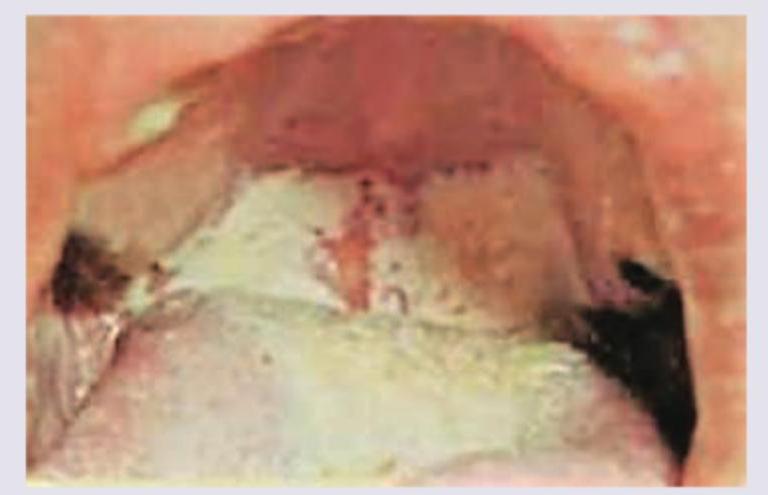
A 70 year old man with history of smoking has a 1 cm ulcerative lesion over the vermilion of his upper lip. What is he likely to be suffering from?
A 65-year-old man presents with a slowly growing, hyperkeratotic lesion on his right temple. The lesion has been present for approximately 8 months. He has a history of significant sun exposure. Examination reveals a 1.5 cm scaly, erythematous plaque with adherent scale. Biopsy shows atypical keratinocytes extending from the epidermis into the dermis. Which of the following is the most likely diagnosis?
A 55-year-old man with a history of sun exposure presents with a slowly growing, pearly nodule with telangiectasias on his nose. The lesion occasionally bleeds when traumatized. Biopsy shows basaloid cells arranged in palisading patterns. Which of the following mutations is most likely involved in the pathogenesis?
Practice by Chapter
Benign Epithelial Tumors
Practice Questions
Premalignant Epidermal Tumors
Practice Questions
Basal Cell Carcinoma
Practice Questions
Squamous Cell Carcinoma
Practice Questions
Melanocytic Nevi
Practice Questions
Melanoma
Practice Questions
Merkel Cell Carcinoma
Practice Questions
Vascular Tumors and Malformations
Practice Questions
Cutaneous Lymphomas
Practice Questions
Soft Tissue Tumors
Practice Questions
Metastatic Skin Tumors
Practice Questions
Skin Cancer Prevention and Screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app