
Skin Tumors — MCQs

On this page
A 60-year-old person presented with an ulcer on the medial canthus. The ulcer has rolled-out, beaded margins. Histopathology shows nesting cells with peripheral palisading patterns. What is the most likely diagnosis?
A patient presents with a lesion on the sun-exposed area shown in the image. What is the most likely diagnosis?

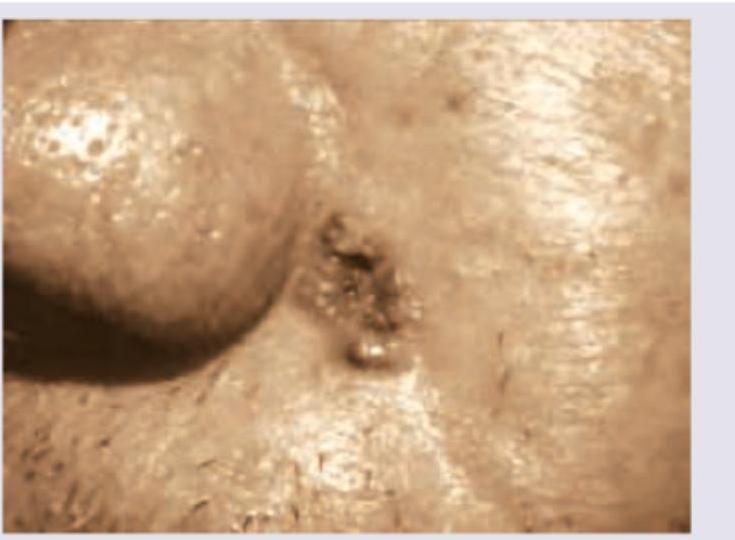
A patient presents with ulcer on the side of the nose, as shown, which bleeds on itching. What is the diagnosis? (AIIMS Nov 2017)
What is true regarding the picture shown below?

What is true regarding the picture shown below? (Biopsy of this lesion demonstrated basaloid nests with peripheral palisading and stromal retraction, confirming basal cell carcinoma.)

The image given below shows:

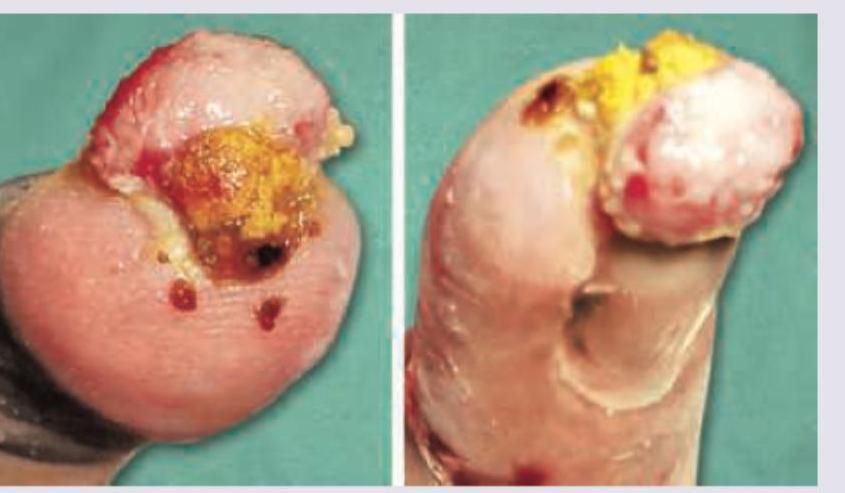
A 30-year-old construction worker had a partial traumatic nail avulsion. 3 weeks later he presents with the presentation shown below. What is the diagnosis?
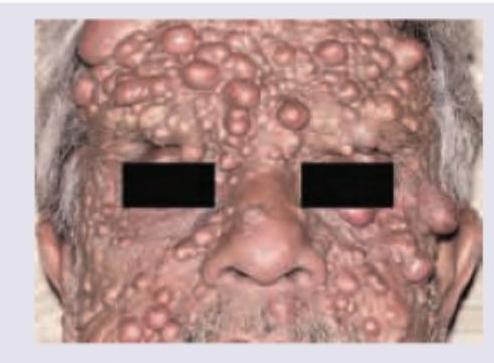
What is the diagnosis based on the clinical image shown?
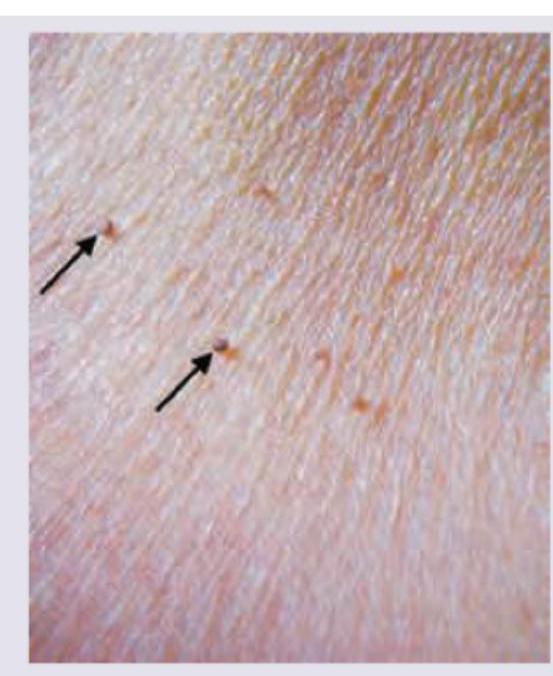
The following image shows presence of:
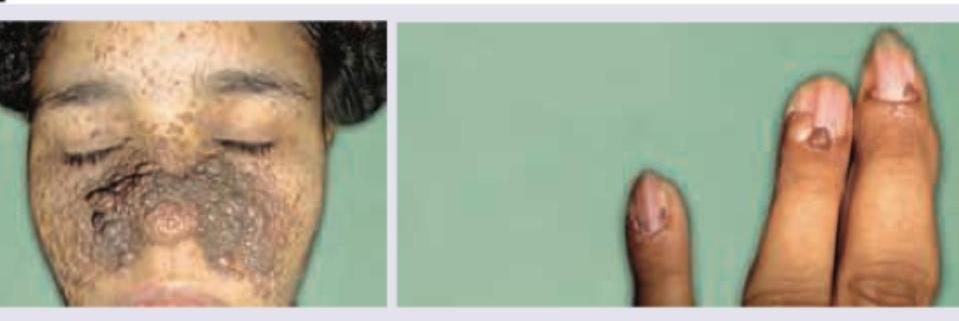
The image shows presence of:
Practice by Chapter
Benign Epithelial Tumors
Practice Questions
Premalignant Epidermal Tumors
Practice Questions
Basal Cell Carcinoma
Practice Questions
Squamous Cell Carcinoma
Practice Questions
Melanocytic Nevi
Practice Questions
Melanoma
Practice Questions
Merkel Cell Carcinoma
Practice Questions
Vascular Tumors and Malformations
Practice Questions
Cutaneous Lymphomas
Practice Questions
Soft Tissue Tumors
Practice Questions
Metastatic Skin Tumors
Practice Questions
Skin Cancer Prevention and Screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app