
Vitiligo — MCQs

Match the following woods lamp findings: 1. Erythrasma, 2. Pityriasis versicolor, 3. Tinea capitis, 4. Vitiligo || a. Yellow b. Coral red fluorescence c. Pink d. Green e. Milky white
A child comes with a circular 3cm x 3cm scaly patchy hair loss with itching in the lesions. The investigation of choice is
PUVA therapy is used in all except:
Large unilateral hypopigmented lesions on the right trunk and arm in a female are best explained by which of the following?
Koebner's phenomenon is seen in all except
Koebner's phenomenon seen in ?
"Isomorphic response" can be a feature of the following except
A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
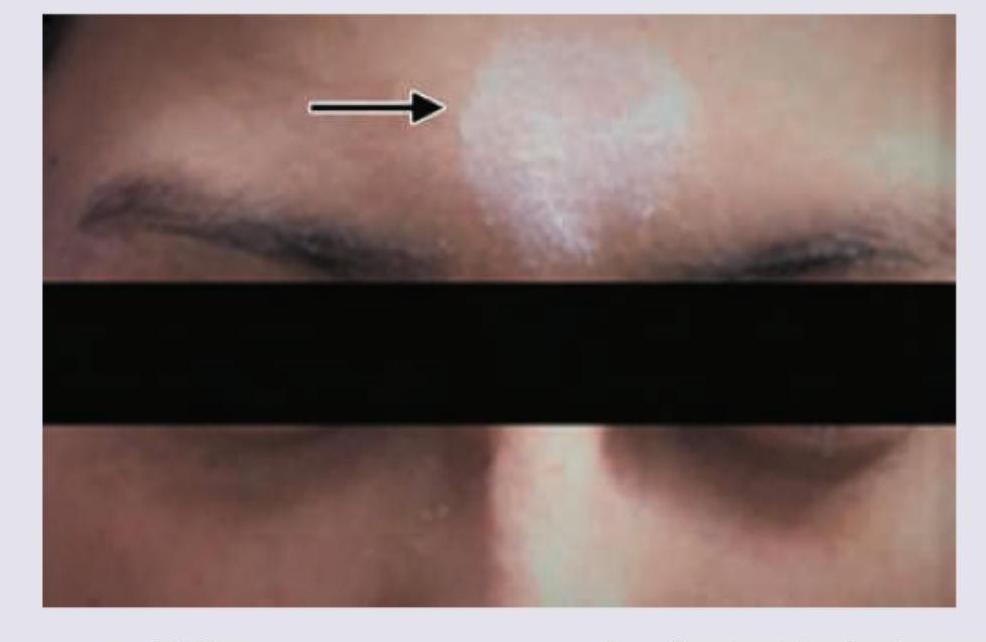
A young girl presents with leukotrichia and lesions as shown in the image. What is the most likely diagnosis?

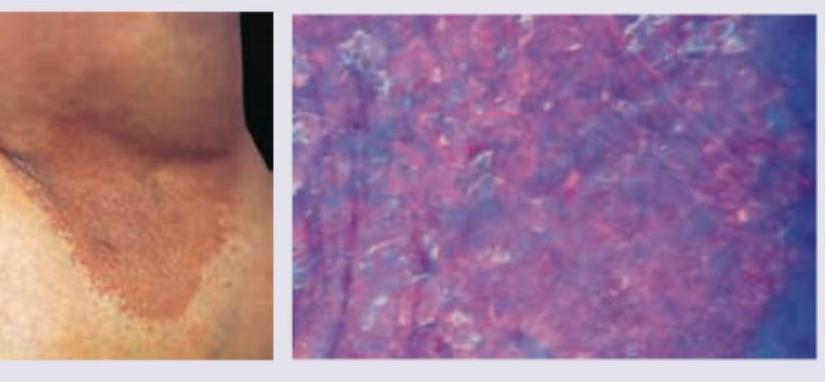
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app