
Post-inflammatory Hypopigmentation — MCQs

Match the following woods lamp findings: 1. Erythrasma, 2. Pityriasis versicolor, 3. Tinea capitis, 4. Vitiligo || a. Yellow b. Coral red fluorescence c. Pink d. Green e. Milky white
What is the primary condition for which calcitriol is used as a treatment?
Contraindications for skin traction: a) Dermatitis b) Vascularly compromised status of limb c) Abrasions d) Hypopigmentation (vitiligo) e) Bony deformity
How does narrowband UVB therapy work in psoriasis?
Large unilateral hypopigmented lesions on the right trunk and arm in a female are best explained by which of the following?
A 15cm hyperpigmented macule on an adolescent male undergoes changes such as coarseness, growth of hair & acne. Diagnosis is?
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
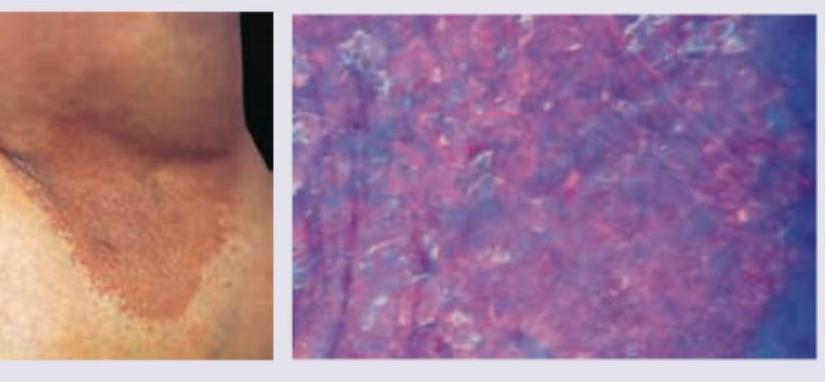
Which of the following is not a part of P. versicolor treatment -
Match the following scale types with their lesions. | Scales | Lesions | | :-- | :-- | | 1. Collarette scales | a. Pityriasis versicolour | | 2. Silvery scales | b. Pityriasis rosea | | 3. Mica-like scales | c. Psoriasis | | 4. Branny scales | d. Pityriasis lichenoides |
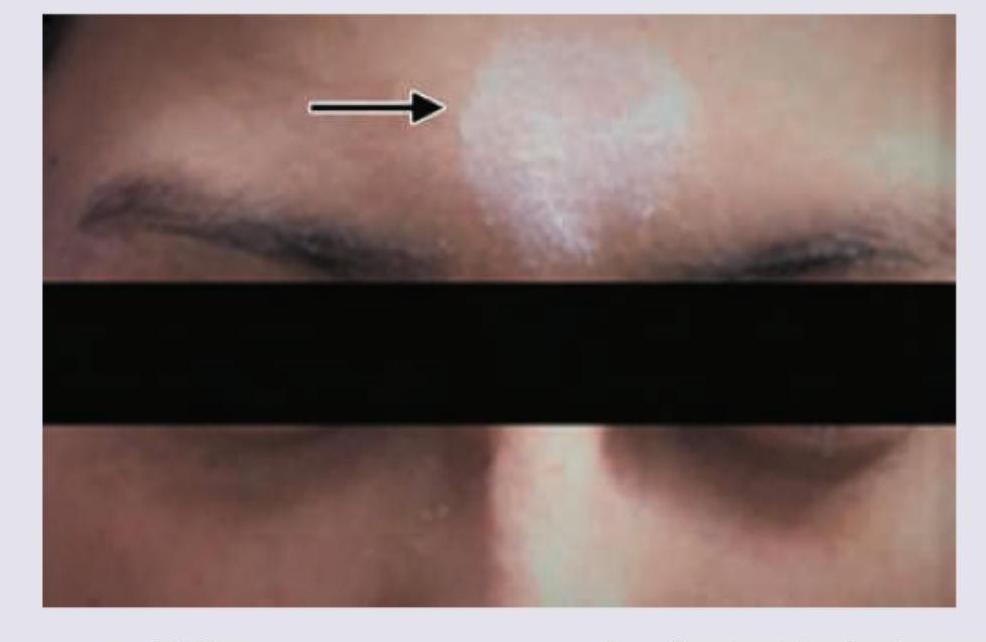
A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app