
Post-inflammatory Hyperpigmentation — MCQs

Mycosis fungoides primarily involves which type of immune cell?
False about Tinea versicolor
Recalcitrant acne is treated by:
A 35 years old female presented with acne. She was treated for her acne but after the treatment, she developed pigmentation. Which drug is responsible for hyperpigmentation?
Dermatological manifestation of which of the following diseases?

Which of the following is not true about hydroquinone?
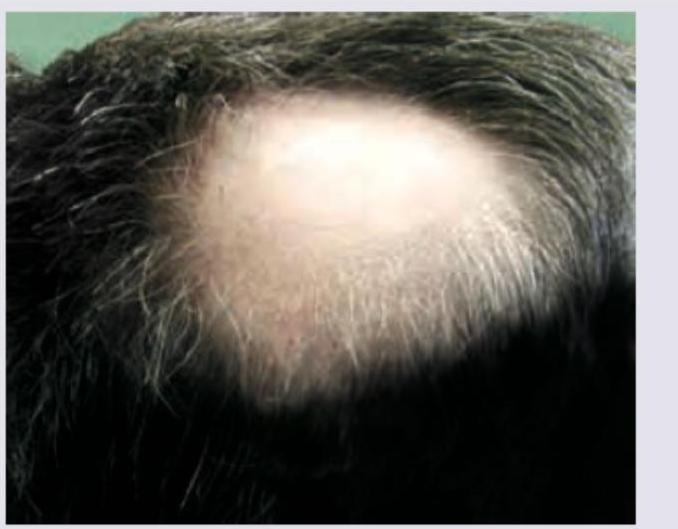
In a patient with the following lesion on scalp, what changes are seen in the nails?
In which of the following conditions is the Koebner phenomenon most commonly observed?
A 50-year-old man with Fitzpatrick skin type V desires treatment for melasma. He was previously treated with triple combination cream with partial response. What would be the most evidence-based next step considering safety and efficacy?
What is the most common association with Acanthosis nigricans?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app