
Pigmentary Disorders — MCQs

On this page
The image shows presence of:
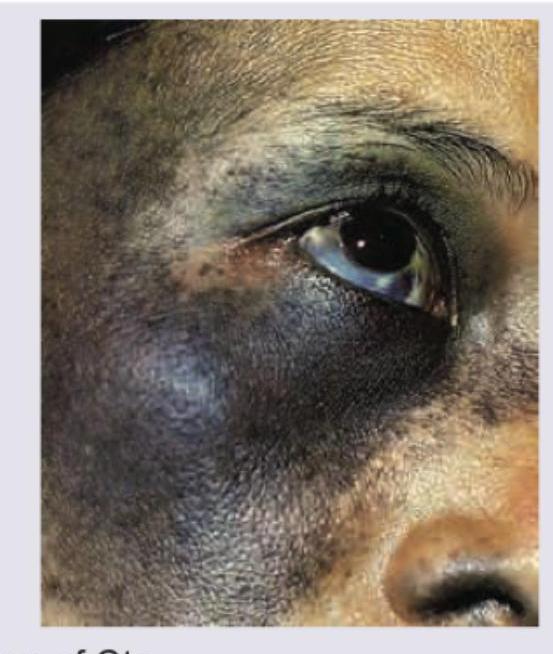
A 24-year-old male presents with a lesion at the site shown in the image for 4 years. He says it has increased in thickness over the years. Diagnosis is:

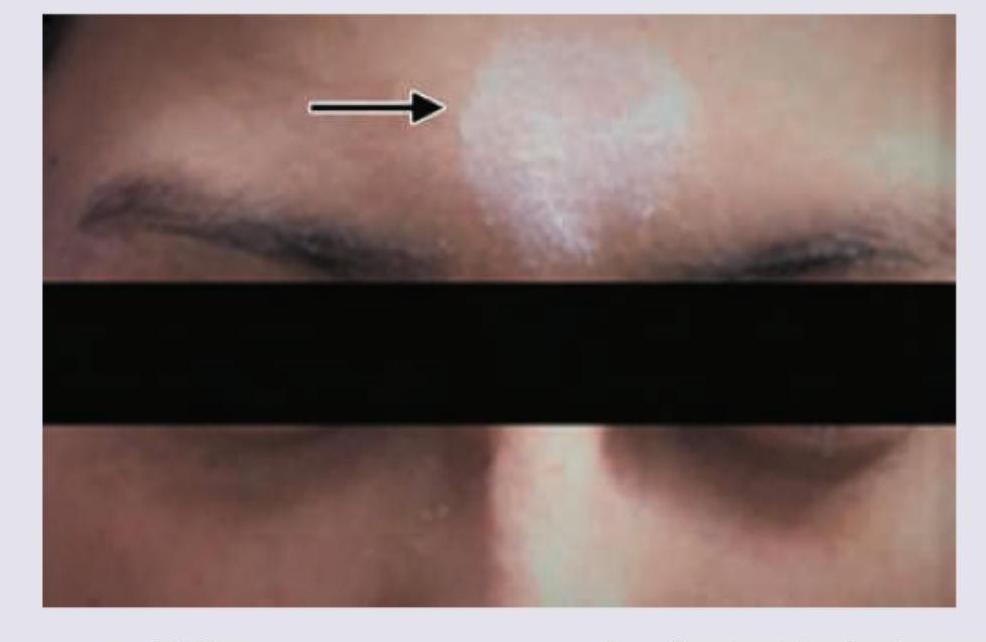
A patient presents with the skin finding shown in the image. The depigmented patch on the forehead and a white forelock have been present since birth and have remained stable. Identify the most likely diagnosis for this lesion.
The clinical diagnosis is?

The image shows Bilateral Xanthelasma palpebrarum. Which of the following is the most common type of xanthoma?
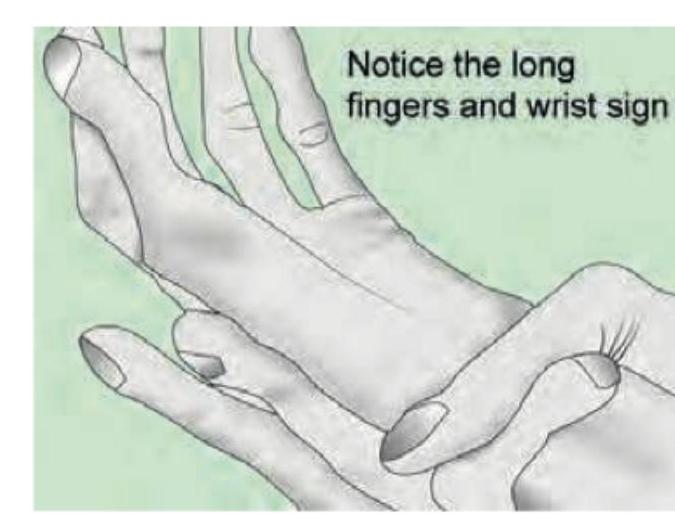
Consider the following statements regarding oculocutaneous albinism : I. The disease results from genetic abnormalities leading to destruction of melanocytes II. Type 1 albinism is due to a defect in the tyrosinase gene III. Patients may present with poor vision, rotator nystagmus and alternating strabismus IV. Patients are at an increased risk of sunburn or developing skin cancer Which of the statements given above are correct?
A young girl presents with leukotrichia and lesions as shown in the image. What is the most likely diagnosis?

A 28-year-old woman presents with progressive darkening of her face that started during pregnancy. The pigmentation is symmetrical and primarily affects her cheeks and forehead. It became more prominent with sun exposure. Examination reveals bilateral, symmetrical brown patches on her face. Which of the following is the most appropriate initial management?
An 18-year-old woman was diagnosed 7 years earlier with precocious pseudopuberty secondary to ovarian tumor. Physical examination reveals oral and lingual dark pigmentation. (See Figure below). Which of the following is the most likely diagnosis?

Which of the following is not true about hydroquinone?
Practice by Chapter
Melanocyte Biology
Practice Questions
Vitiligo
Practice Questions
Melasma
Practice Questions
Post-inflammatory Hyperpigmentation
Practice Questions
Post-inflammatory Hypopigmentation
Practice Questions
Albinism
Practice Questions
Drug-Induced Pigmentary Changes
Practice Questions
Pityriasis Alba
Practice Questions
Pigmentary Demarcation Lines
Practice Questions
Nevi of Ota and Ito
Practice Questions
Management of Hyperpigmentation
Practice Questions
Management of Hypopigmentation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app