
Pigmentary Disorders — MCQs

On this page
Which of the following is the reason for the development of a simple lentigo?
Hypopigmented patches can be seen in which of the following conditions?
A female developed a brown macule on the cheek, forehead, and nose after exposure to light following delivery of a baby. What is the diagnosis?
A 20-year-old patient presents with a non-progressive hypopigmented lesion on the trunk. On Wood's lamp examination, there is white accentuation. Diascopy is negative. What is the most likely diagnosis?
A 13-year-old boy presents with patchy depigmented skin on the right flank and upper thigh in segmental distribution, as shown in the image. The depigmentation started 1 year back but has been static for last 4 months. Mother reports use of topical steroids which was ineffective. Diagnosis is?

An 18-year-old female presents with sharply demarcated depigmented patches on the dorsal aspect of the foot, consistent with vitiligo. Which of the following drugs should not be used in the treatment of this patient? (AIIMS May 2016)

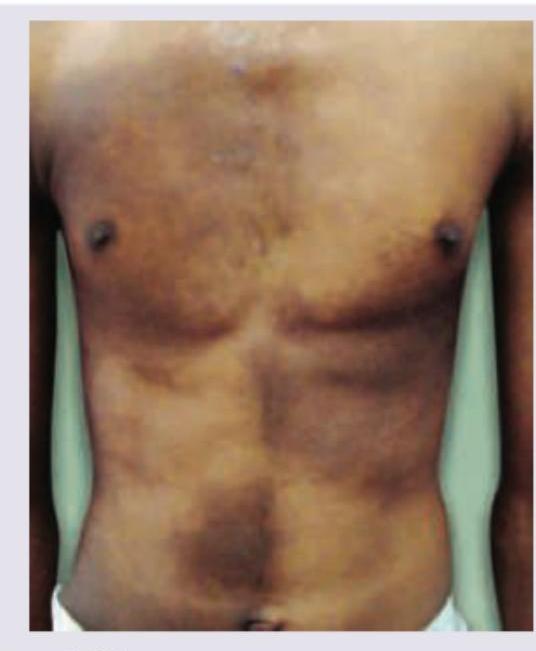
The given image shows:

A patient presents with congenital, stable depigmented patches present since birth. The image shows presence of:

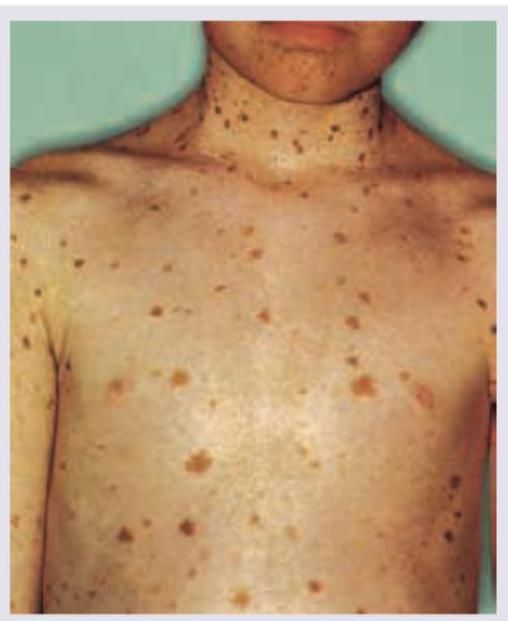
The image shows presence of:
The image shows presence of:
Practice by Chapter
Melanocyte Biology
Practice Questions
Vitiligo
Practice Questions
Melasma
Practice Questions
Post-inflammatory Hyperpigmentation
Practice Questions
Post-inflammatory Hypopigmentation
Practice Questions
Albinism
Practice Questions
Drug-Induced Pigmentary Changes
Practice Questions
Pityriasis Alba
Practice Questions
Pigmentary Demarcation Lines
Practice Questions
Nevi of Ota and Ito
Practice Questions
Management of Hyperpigmentation
Practice Questions
Management of Hypopigmentation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app