
Melasma — MCQs

Elderly man with a long-standing mole on his face that is increasing in size and showing an irregular border. Diagnosis:
All are predisposing factors of Deep Vein thrombosis, EXCEPT :
PUVA therapy is used in all except:
Which of the following is not true about hydroquinone?
Which of the following is an example of a barrier method of contraception?
A 15cm hyperpigmented macule on an adolescent male undergoes changes such as coarseness, growth of hair & acne. Diagnosis is?
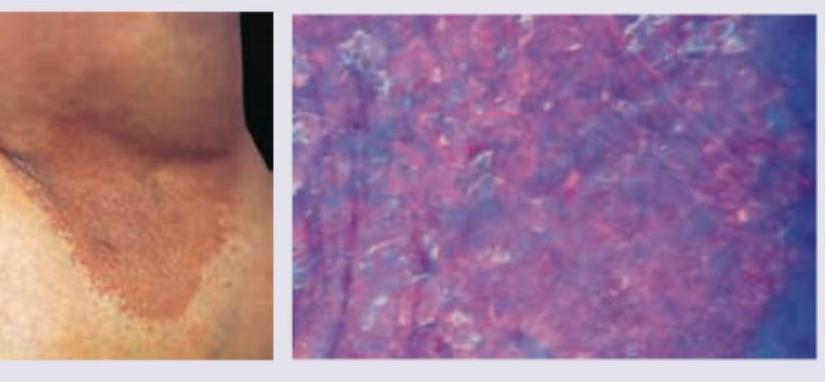
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
A 50-year-old man with Fitzpatrick skin type V desires treatment for melasma. He was previously treated with triple combination cream with partial response. What would be the most evidence-based next step considering safety and efficacy?
What is the most common association with Acanthosis nigricans?
An increased incidence of vitiligo is found in association with which of the following conditions?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app