
Management of Hypopigmentation — MCQs

Which drug is generally contraindicated in the management of traumatic hyphema in a patient with sickle cell disease?
An adult presents with oval, scaly, hypopigmented macules over the chest and back. The diagnosis is
Which of the following strategies are part of the National Leprosy Control Programme?
All of the following are used in systemic therapy of psoriasis except
Multiple hypoaesthetic, hypopigmented macules on right lateral forearm with numerous acid-fast bacilli is indicative of:
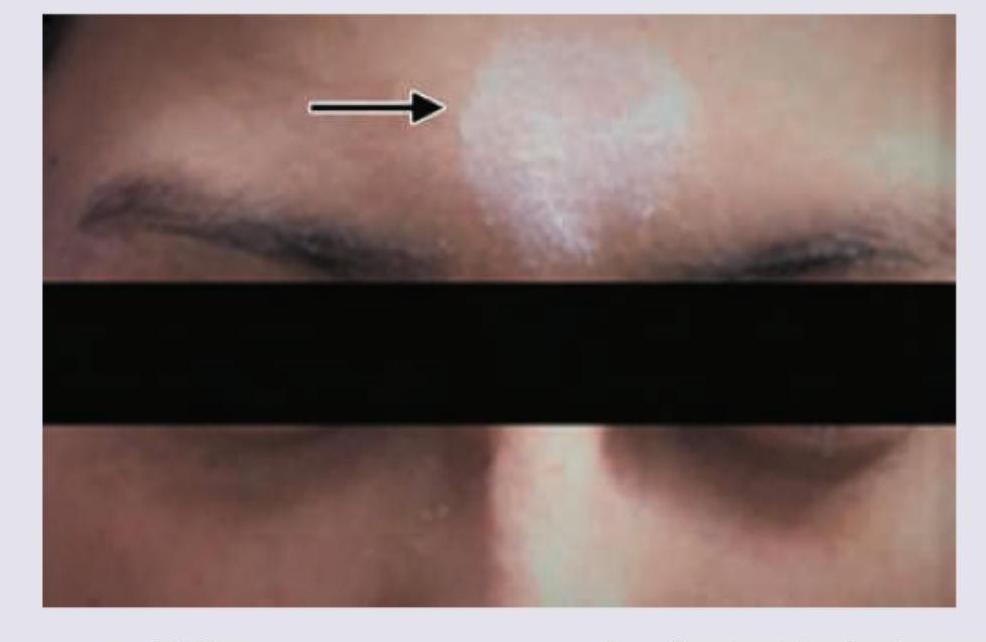
A young girl presents with leukotrichia and lesions as shown in the image. What is the most likely diagnosis?

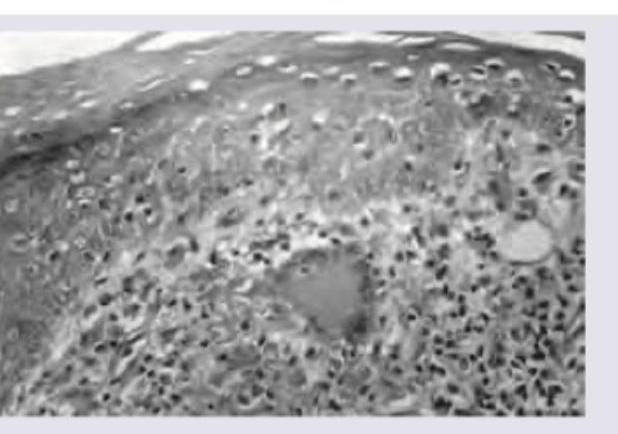
A young male presented with an anesthetic patch on the right forearm. A thickened nerve was palpable on examination. Skin biopsy shows the image below. What is the diagnosis?
A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
A 50-year-old man with Fitzpatrick skin type V desires treatment for melasma. He was previously treated with triple combination cream with partial response. What would be the most evidence-based next step considering safety and efficacy?
What is the most common association with Acanthosis nigricans?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app