
Parasitic Skin Infections — MCQs

On this page
What is considered the most severe form of scabies?
Skin lesions following visceral leishmaniasis typically present as which of the following?
The Circle of Hebra is associated with which of the following conditions?
In an infant with scabies, what is the preferred treatment?
Which of the following drugs is useful for the following condition? (Recent NEET Pattern 2016-17)

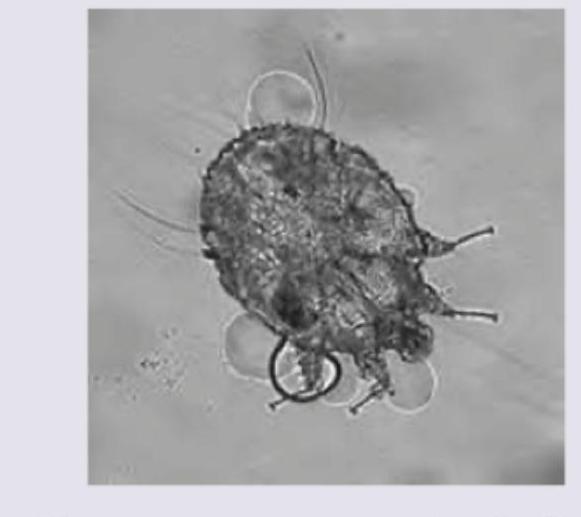
An AIDS positive patient has presented with multiple crusted lesions as shown in the image below. What is the possible diagnosis?

A patient lives in an urban slum and walks barefoot on soil contaminated by dog or cat feces. He presented with continuous itching over the sole. The image shows presence of:

A middle-aged man came to you with itchy rash caused by the following organism. Identify the condition: (AIIMS Nov 2017)
Which of the following statements about pediculosis pubis is MOST accurate?
Which physical finding is most useful in diagnosing scabies in genital lesions?
Practice by Chapter
Scabies
Practice Questions
Pediculosis
Practice Questions
Cutaneous Larva Migrans
Practice Questions
Leishmaniasis
Practice Questions
Onchocerciasis
Practice Questions
Myiasis
Practice Questions
Tungiasis
Practice Questions
Cutaneous Amebiasis
Practice Questions
Cutaneous Manifestations of Malaria
Practice Questions
Ectoparasitic Infestations
Practice Questions
Diagnosis of Parasitic Infestations
Practice Questions
Antiparasitic Therapy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app