
Telogen Effluvium — MCQs

HR-180, BP-60/40, temp-39.5°C, ETCO2-65 post induction. Most likely diagnosis:
A 22-year-old woman presents with diffuse hair loss for 1 month. She had a past history of enteric fever 4 months ago. What is the likely cause?
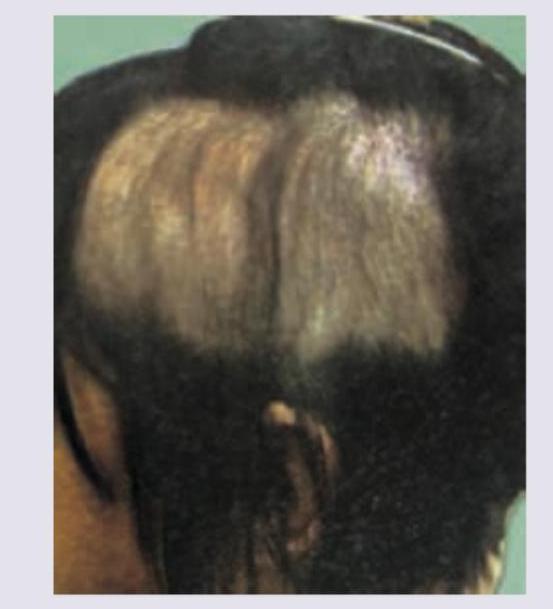
The following patient presented to the OPD with history of hair loss. There was no erythema, scarring or scratching. Diagnosis is:
Rapid, diffuse, excessive hair loss occurring 3 months after childbirth is due to?
A male presents with alopecia and exclamation mark hairs. Diagnosis?
A female presented with complaints of hair fall. Her delivery was 2 months ago. Physician diagnosed her condition as Telogen Effluvium. All of the following are true regarding telogen effluvium, EXCEPT:
A male presents with alopecia and exclamation mark hairs. Diagnosis?
Swarm of bees appearance seen in?
Non-scarring alopecia is associated with all except?
Consider the following causes of alopecia: 1. Androgenetic alopecia 2. Alopecia areata 3. Telogen effluvium 4. Lichen planopilaris. Which among the following causes non-scarring alopecia?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app