
Hair and Nail Disorders — MCQs

On this page
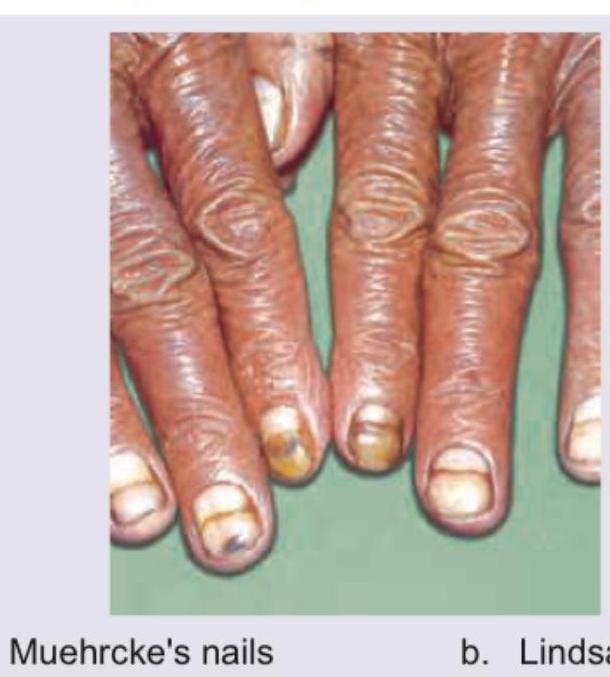
The image shows presence of:

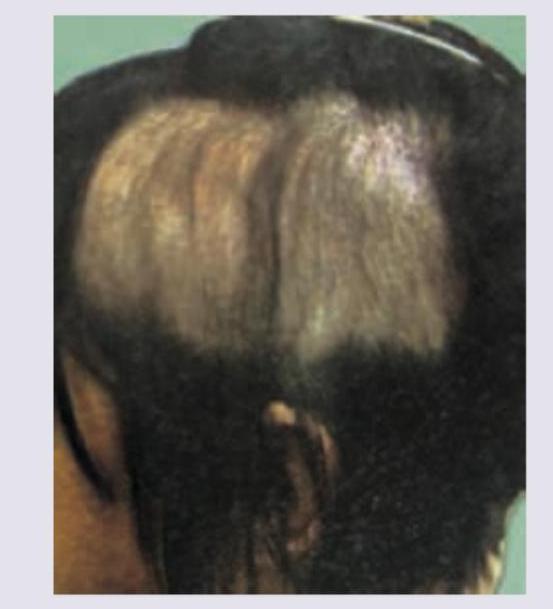
The image shows presence of:

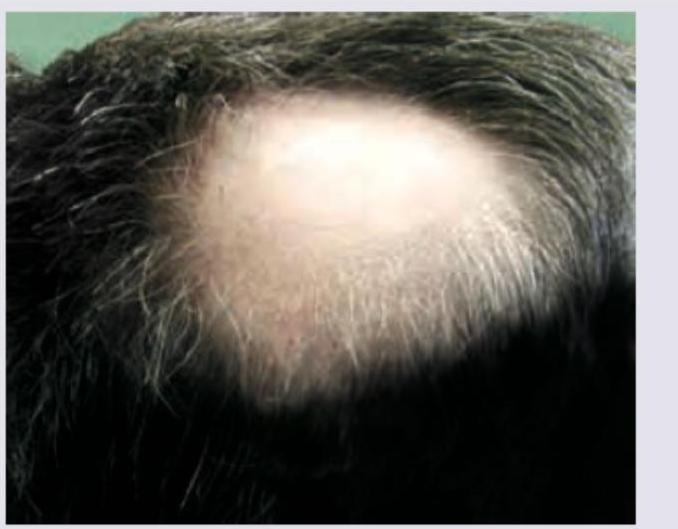
The image shows presence of:
The following patient presented to the OPD with history of hair loss. There was no erythema, scarring or scratching. Diagnosis is:
The nail lesion shown in the image is known as?

In a patient with the following lesion on scalp, what changes are seen in the nails?
Consider the following regarding the human hair growth cycle : I. Anagen is a phase of active hair growth II. Telogen is a transitional phase III. Catagen is a resting phase Which of the statements given above is/are correct?
Consider the following causes of alopecia: 1. Androgenetic alopecia 2. Alopecia areata 3. Telogen effluvium 4. Lichen planopilaris. Which among the following causes non-scarring alopecia?
Non-scarring alopecia is associated with all except?
Nails are involved in all except:
Practice by Chapter
Hair Growth Cycle and Anatomy
Practice Questions
Alopecia Areata
Practice Questions
Androgenetic Alopecia
Practice Questions
Telogen Effluvium
Practice Questions
Scarring Alopecias
Practice Questions
Hair Shaft Abnormalities
Practice Questions
Hirsutism and Hypertrichosis
Practice Questions
Nail Anatomy and Growth
Practice Questions
Nail Infections
Practice Questions
Nail Psoriasis and Other Inflammatory Nail Disorders
Practice Questions
Nail Tumors
Practice Questions
Management of Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app