
Hair and Nail Disorders — MCQs

On this page
Nail pitting is associated with all of the following conditions except?
A patient presents with scarring alopecia, thinned nails, and hypopigmented macular lesions over the trunk and oral mucosa. What is the diagnosis?
The Hamilton Norwood scale is used for assessing the extent of which condition?
The "half-and-half" nail or "half-nail" sign, seen in uremia, is primarily caused by which of the following?
A 35-year-old male presents with bald patches and no scars. The patches are well demarcated with broken hair at the edges. What is the diagnosis?
Which of the following drugs does NOT cause hirsutism?
What is the most likely diagnosis in this 50-year-old woman?
Androgenic alopecia in females is caused by which of the following conditions?
An elderly female undergoing chemotherapy for breast cancer is experiencing significant hair loss. What is the most likely cause of her condition?
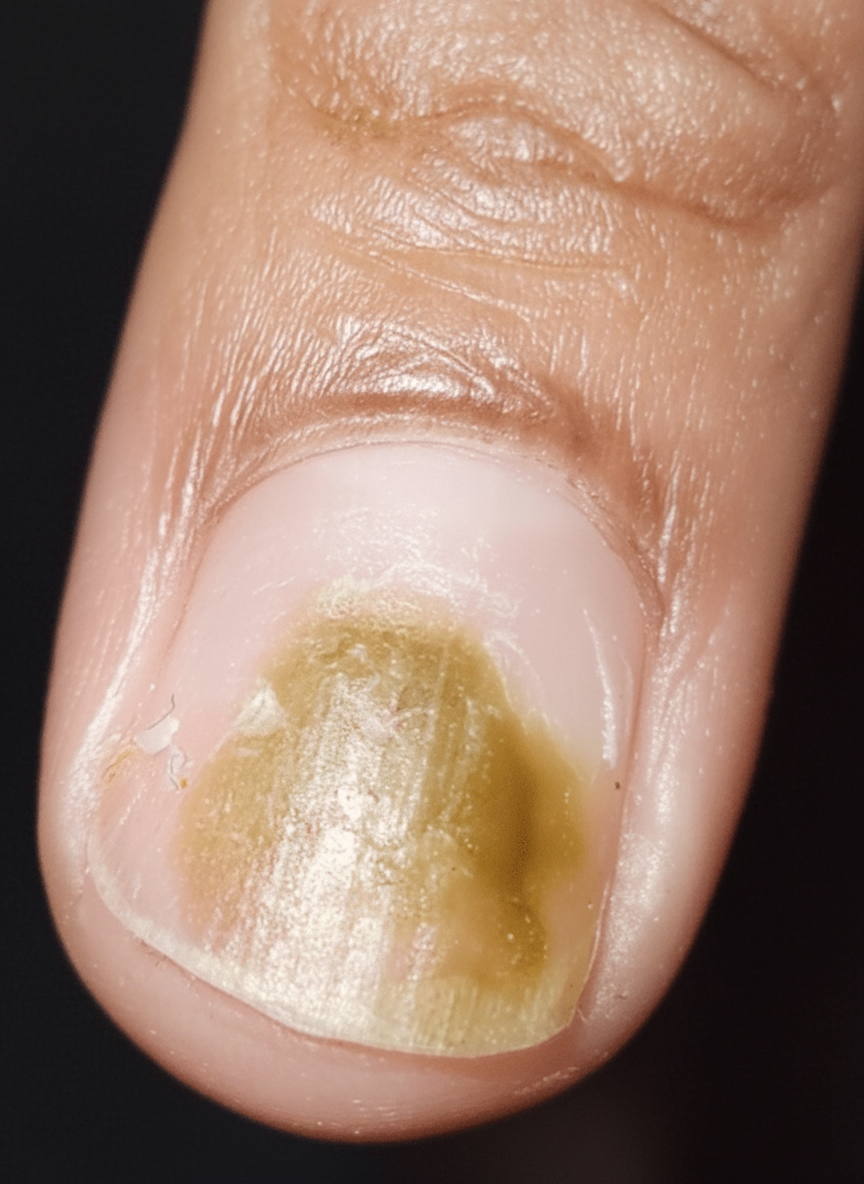
Identify the lesion: (Recent NEET Pattern 2016-17)

Practice by Chapter
Hair Growth Cycle and Anatomy
Practice Questions
Alopecia Areata
Practice Questions
Androgenetic Alopecia
Practice Questions
Telogen Effluvium
Practice Questions
Scarring Alopecias
Practice Questions
Hair Shaft Abnormalities
Practice Questions
Hirsutism and Hypertrichosis
Practice Questions
Nail Anatomy and Growth
Practice Questions
Nail Infections
Practice Questions
Nail Psoriasis and Other Inflammatory Nail Disorders
Practice Questions
Nail Tumors
Practice Questions
Management of Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app