
Dermatological Pharmacology — MCQs

On this page
A 20-year-old patient with focal seizures was prescribed Carbamazepine. Four weeks later he presents with fever and multiple skin lesions with periorbital edema. On examination generalized lymph nodes enlargement is noted. Blood work shows marked eosinophilia with atypical lymphocytosis. What is the diagnosis?
A 30-year-old Han Chinese woman with multiple episodes of GTCS was prescribed phenytoin by district hospital physician. After 7 days she presents with fever, malaise, mucosal erosions involving the oral and conjunctival mucosa, and widespread skin involvement with epidermal detachment. Which of the following will predispose to the condition shown here? (Recent NEET Pattern 2016-17)

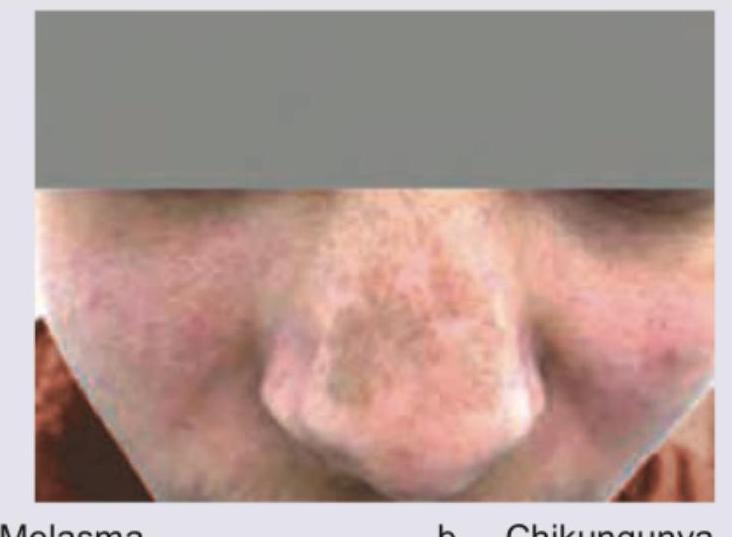
A patient presented with fever and joint pain for which she was put on NSAIDs. After 10 days she developed a skin lesion as shown in the image. The lesion is bilateral, symmetrical, and centrofacially distributed over the nose and malar regions, without any preceding dusky erythematous plaque and not confined to a single sharply demarcated site. Diagnosis is:

A 30-year-old male presents with joint pain and NSAIDs were prescribed. After one week, joint pain is persisting and he has developed brownish discoloration over nose as shown in the figure. The nasal discoloration was not preceded by any localized erythematous or inflamed lesion, and there is no prior history of a similar lesion at the same site. This was due to: (AIIMS Nov 2017)
FTU is a measure of:
Steroids are used in the Rx of the following diseases EXCEPT:
A 35 years old female presented with acne. She was treated for her acne but after the treatment, she developed pigmentation. Which drug is responsible for hyperpigmentation?
Match the systemic medications with their most characteristic cutaneous adverse effects: 1. Hydroxyurea a. Acral erythema 2. Capecitabine b. Leg ulcers 3. EGFR inhibitors c. Acneiform eruption
Which mechanism best explains the therapeutic effect of coal tar in psoriasis?
A 50-year-old woman presents with a well-defined erythematous patch on her leg following the administration of an antibiotic. What is the most likely diagnosis?
Practice by Chapter
Topical Corticosteroids
Practice Questions
Topical Antibiotics
Practice Questions
Topical Antifungals
Practice Questions
Topical Antivirals
Practice Questions
Topical Retinoids
Practice Questions
Systemic Retinoids
Practice Questions
Immunosuppressive Agents
Practice Questions
Antihistamines in Dermatology
Practice Questions
Biological Agents in Dermatology
Practice Questions
Dermatological Vehicles and Delivery Systems
Practice Questions
Phototherapeutic Agents
Practice Questions
Adverse Cutaneous Drug Reactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app