
Dermatological Pharmacology — MCQs

On this page
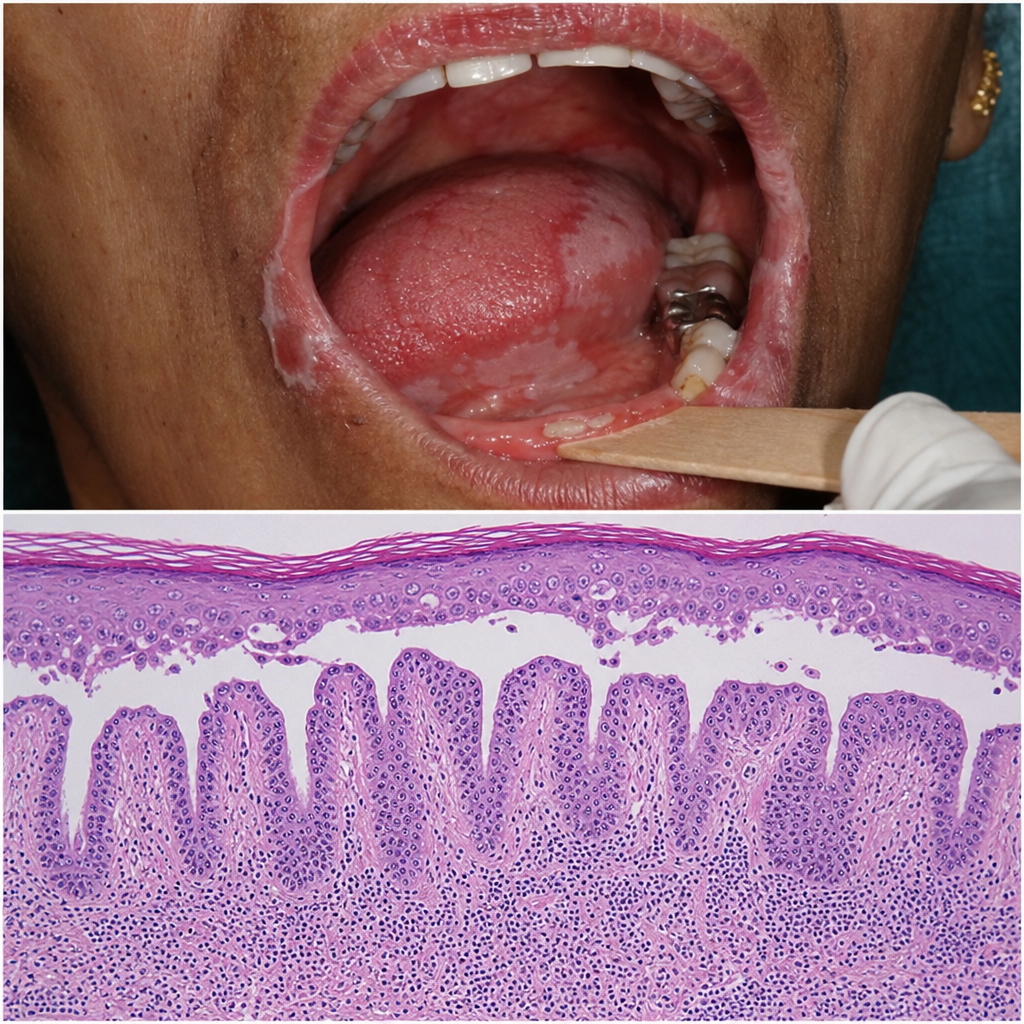
A 55-year-old woman presents with painful oral erosions and minimal skin involvement for 3 months. Nikolsky sign is positive on the oral mucosa. Serum is sent for autoantibody testing. Histology of a perilesional biopsy shows suprabasal acantholysis with a tombstone row of basal keratinocytes (Image). In this predominantly mucosal variant of pemphigus vulgaris, which autoantibody titre best correlates with mucosal disease activity and guides decisions about tapering systemic immunosuppression?
A 24-year-old man presents to the emergency department with a 3-day history of a rapidly spreading rash on his hands and forearms. He had a cold sore on his lip 10 days ago. He denies any new medications. There is no mucosal involvement. The rash is shown (Image 2). Which of the following statements best describes the underlying immunopathological mechanism responsible for this eruption?

Dapsone is used in which of the following conditions?
A male presents with an erythematous patch over the penis after taking an over-the-counter medication. What is the most likely causal drug?
Which of the following antifungal drugs is developing drug resistance and has not been prescribed for tinea cruris and tinea corporis for the last 2 years?
All are drugs known to be associated with drug hypersensitivity syndrome, EXCEPT:
Which of the following is given in the form of an intralesional injection to treat keloid?
Which of the following is NOT a drug-induced cause of Addison's disease?
What is the drug of choice for Type II Lepra Reaction?
All of the following are side effects of topical steroids EXCEPT:
Practice by Chapter
Topical Corticosteroids
Practice Questions
Topical Antibiotics
Practice Questions
Topical Antifungals
Practice Questions
Topical Antivirals
Practice Questions
Topical Retinoids
Practice Questions
Systemic Retinoids
Practice Questions
Immunosuppressive Agents
Practice Questions
Antihistamines in Dermatology
Practice Questions
Biological Agents in Dermatology
Practice Questions
Dermatological Vehicles and Delivery Systems
Practice Questions
Phototherapeutic Agents
Practice Questions
Adverse Cutaneous Drug Reactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app