
Seborrheic Dermatitis — MCQs

A child presenting with localized patches of complete hair loss with normal appearance of scalp. The diagnosis is:
Match the following scale types with their lesions. | Scales | Lesions | | :-- | :-- | | 1. Collarette scales | a. Pityriasis versicolour | | 2. Silvery scales | b. Pityriasis rosea | | 3. Mica-like scales | c. Psoriasis | | 4. Branny scales | d. Pityriasis lichenoides |
Skin biopsy shows psoriasiform hyperplasia with neutrophilic microabscesses in stratum corneum. Most likely diagnosis?
Which of the following is used in the treatment of Pityriasis versicolor?
An eleven-year-old boy has Tinea capitis on his scalp. Which of the following is the most appropriate line of treatment for this condition?
An 8-year-old child has localized non-cicatricial alopecia over scalp with itching and scales. The diagnosis is :
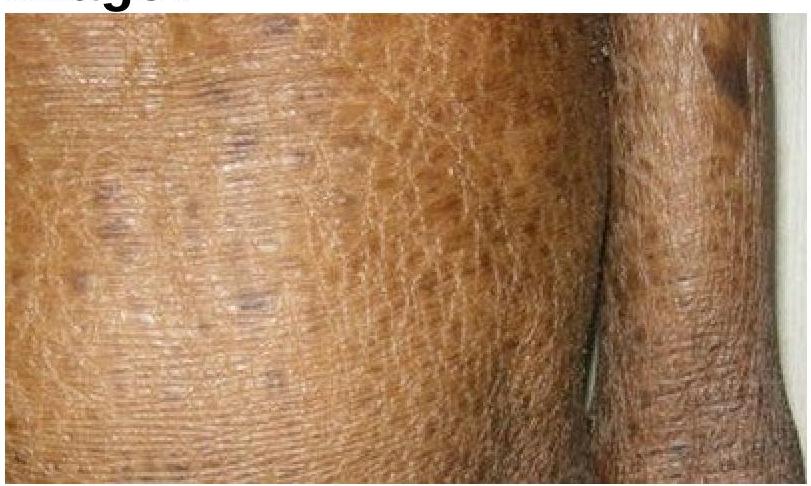
Identify the skin condition depicted in the image.
Which of the following organisms has a role to play in Seborrheic dermatitis?
Pompholyx affects:
A child presented with itchy plaques over the neck, the bilateral popliteal and cubital fossa. What could be the diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app